Glomerular Filtration Rate (GFR)
GFR (mL/min/1.73 m2) = 175 × (Scr)-1.154 × (Age)-0.203 × (0.742 if female) × (1.212 if African American)
The equation does not require weight or height variables because the results are reported normalized to 1.73 m2 body surface area, which is an accepted average adult surface area.
Scr = Serum Creatinine level
Reference:
Related Calculators
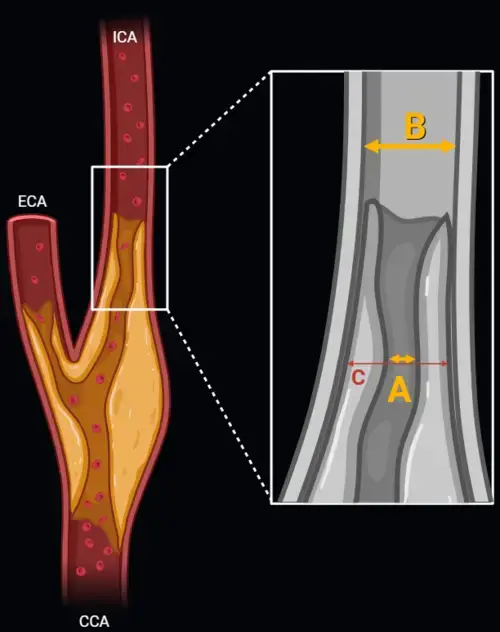
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
Prostate volume estimation with PSA density calculation using imaging measurements and serum PSA levels.
Differentiation of adrenal adenomas using absolute and relative washout measurements on contrast-enhanced CT.
Thyroid nodule risk stratification using ultrasound features and ACR TI-RADS scoring system.
More about the GFR Calculator and CKD Classification:
Glomerular Filtration Rate (GFR) is the most universally accepted marker for evaluating renal function. Estimating GFR enables clinicians to stage chronic kidney disease (CKD), adjust medication dosages, monitor disease progression, and determine timing for nephrology referral. Our GFR Calculator is based on the well-established MDRD (Modification of Diet in Renal Disease) Study equation and helps streamline these essential clinical tasks in both outpatient and inpatient settings.
The MDRD formula remains a cornerstone in nephrology for estimating kidney function, especially in patients with moderate to advanced CKD. It uses four core variables — serum creatinine, age, sex, and race — to generate an adjusted GFR standardized to a body surface area of 1.73 m². While newer models like CKD-EPI have gained popularity, MDRD remains deeply integrated into clinical workflows and laboratory reports worldwide.
Understanding the MDRD Equation
The MDRD equation provides a reliable method to estimate GFR based on routine lab data and basic demographics. It is particularly suited for individuals with impaired kidney function and is less reliable for those with normal or near-normal GFR values.
- Serum Creatinine (mg/dL): A key marker of kidney function.
- Age: Renal function naturally declines with age.
- Sex: Adjusts for average muscle mass differences.
- Race: Adjusts for higher creatinine generation in Black individuals.
MDRD Formula:
GFR (mL/min/1.73 m²) = 175 × (Serum Creatinine)^–1.154 × (Age)^–0.203 × (0.742 if female) × (1.212 if Black)
Clinical Utility of GFR Estimation
Accurate GFR calculation is fundamental for:
- Detecting and classifying CKD early
- Preventing complications from medication toxicity
- Evaluating contrast nephropathy risk in imaging
- Identifying candidates for dialysis or transplant evaluation
- Monitoring effectiveness of lifestyle or pharmacologic interventions
In primary care, nephrology, and radiology settings, the GFR estimate empowers clinicians to personalize treatment decisions. The tool's ease of use also supports widespread screening in high-risk populations such as diabetics, hypertensives, and elderly patients.
CKD Stages Based on GFR
CKD is classified into stages according to GFR, with each stage associated with specific risks and management strategies. The earlier the detection, the greater the opportunity to slow or halt disease progression.
- Stage 1: GFR ≥ 90 (with evidence of kidney damage)
- Stage 2: GFR 60–89
- Stage 3a: GFR 45–59
- Stage 3b: GFR 30–44
- Stage 4: GFR 15–29
- Stage 5: GFR < 15 (End-stage renal disease / dialysis candidate)
CKD staging also guides frequency of follow-up, laboratory surveillance, and patient education efforts. Our calculator provides automatic stage classification to help standardize decision-making.
When to Use the GFR Calculator
Routine use of GFR estimation is encouraged in a variety of scenarios:
- Screening asymptomatic individuals with risk factors
- Assessing chronic comorbidities such as heart failure or diabetes
- Adjusting doses of medications like metformin, ACE inhibitors, or chemotherapeutic agents
- Determining candidacy for iodinated or gadolinium-based contrast administration
- Documenting longitudinal changes in renal function
Using the GFR calculator during annual checkups can identify silent CKD before irreversible damage occurs, and it can support earlier lifestyle or therapeutic interventions.
MDRD vs CKD-EPI and Other Estimation Models
While MDRD is widely accepted, the CKD-EPI equation has demonstrated greater accuracy at higher GFR values and is increasingly used in academic and tertiary care settings. However, MDRD remains the preferred method in many EMRs and laboratory panels due to its validated performance in patients with moderate to severe kidney disease.
Other estimation methods like the Cockcroft-Gault formula may still be used for drug dosing in specific scenarios, particularly in pharmacokinetics or when actual body weight is a significant variable.
Limitations of the MDRD GFR Calculator
No formula is perfect. GFR estimates assume a steady state of serum creatinine, and all equations have reduced accuracy in the following settings:
- Acute kidney injury (AKI)
- Extremely muscular or malnourished individuals
- Amputees or patients with body composition changes
- Pregnancy
- Unusual dietary intake or creatinine supplements
In these cases, consider direct GFR measurement using radionuclide clearance tests or alternative biomarkers like cystatin C for more accurate results.
GFR and Radiology: Why It Matters
For radiologists and imaging professionals, GFR is essential for evaluating risk prior to contrast-enhanced CT or MRI. A GFR < 30 mL/min/1.73 m² often necessitates special precautions, hydration protocols, or contrast avoidance due to the risk of contrast-induced nephropathy or nephrogenic systemic fibrosis (in the case of gadolinium).
Incorporating a GFR check before scheduling studies not only improves patient safety but also aligns with national guidelines for best practices in imaging. The calculator supports quick decision-making in fast-paced clinical environments.
Integration With Other Clinical Tools
This GFR calculator pairs seamlessly with other decision-support tools across nephrology and radiology. It complements calculators like our adrenal washout CT calculator, used to assess adrenal lesion functionality, and renal trauma grading tools for imaging-based injury staging. Together, they support comprehensive renal care from detection to intervention.
References and Guidelines
Our GFR calculator is aligned with the KDIGO 2012 Clinical Practice Guidelines and is regularly reviewed for compliance with updates in nephrology standards. It is designed to enhance workflow efficiency, improve patient outcomes, and support accurate diagnosis and staging of CKD.
For full guideline reference: KDIGO. (2012). "Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease." Kidney Int Suppl. 2013;3(1):1–150.
