Lung-RADS Calculator v. 2022
A quality assurance tool designed by the American College of Radiology (ACR) to standardize lung cancer screening CT.
Please note: This calculator does not include the "S modifier". Per Lung-RADS® 2022, the S modifier can be added to any categories for clinically significant or potentially clinically significant findings unrelated to lung cancer. This modifier does not affect the follow-up recommendations.
Related Calculators

Coronary artery disease reporting on CT angiography using standardized stenosis severity and reporting categories.

Management of incidental pulmonary nodules on CT based on size, morphology, and patient risk factors.
Thyroid nodule risk stratification using ultrasound features and ACR TI-RADS scoring system.
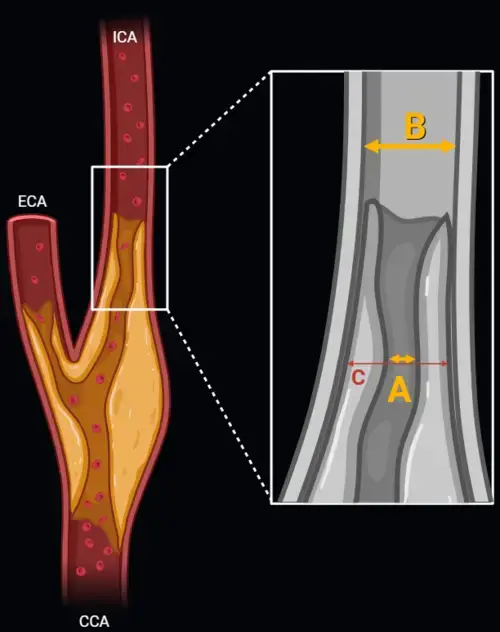
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
More about the Lung-RADS Calculator for categorization of pulmonary lesions
The Lung CT Screening Reporting and Data System (Lung-RADS), developed by the American College of Radiology (ACR), offers a standardized framework for interpreting and managing findings from low-dose computed tomography (LDCT) used in lung cancer screening. First introduced in 2014 and most recently updated in 2022, Lung-RADS provides structured categories to guide follow-up and management strategies based on nodule characteristics and changes over time. This Lung-RADS calculator applies the Lung-RADS version 2022 criteria to help radiologists and clinicians apply these guidelines more easily in routine practice.
Purpose and Scope of Lung-RADS
Lung-RADS is primarily intended for patients undergoing annual lung cancer screening who meet the eligibility criteria established by guidelines, such as age and smoking history. It is not intended for diagnostic CTs performed for symptoms or other clinical indications. By categorizing LDCT findings into a defined set of diagnostic categories, Lung-RADS seeks to minimize ambiguity, clarify risk estimates, and streamline communication with referring providers and patients.
Key Features of Lung-RADS Version 2022
The 2022 update introduced important refinements based on clinical feedback and research evidence. These include more detailed criteria for specific types of nodules and nuanced definitions to better stratify risk:
- Airway-Centered Nodules: Now specifically addressed in the classification to reduce over-calling and clarify follow-up needs.
- Atypical Pulmonary Cysts: Included with defined thresholds for concern, acknowledging their potential role in early lung cancer development.
- Juxtapleural Nodules: Management guidance has been clarified for nodules abutting the pleura, which may have unique behavior and implications.
- Stable or Decreasing Nodules: Growth criteria now include refined definitions for stability and regression, impacting long-term follow-up intervals.
Each of these changes reflects ongoing efforts to improve risk stratification and reduce unnecessary imaging while preserving early detection capabilities.
Lung-RADS Categories and Suggested Management
Lung-RADS categories range from 0 to 4X, reflecting the spectrum from incomplete findings to those requiring more intensive follow-up:
- Category 1: Negative — continue annual screening.
- Category 2: Benign appearance or behavior — continue annual screening.
- Category 3: Probably benign — short-term LDCT follow-up recommended (e.g., 6 months).
- Category 4A: Suspicious — LDCT or PET/CT in 3 months recommended; consider referral.
- Category 4B/4X: Very suspicious — PET/CT, tissue sampling, or other diagnostic evaluation advised.
Recommendations are adjusted based on nodule type (solid, part-solid, ground-glass), size, and change from prior exams. The goal is to intervene appropriately when risk is high while avoiding overtreatment of benign findings.
Why Structured Reporting Matters in Lung Cancer Screening
The use of structured systems like Lung-RADS enhances consistency across radiologists, practices, and institutions. This harmonization is essential not only for accurate clinical care but also for registries, quality assurance, and outcome tracking. Standardization reduces variation in interpretation and ensures that recommendations are tied to established evidence and consensus practices.
Lung-RADS also supports patient-provider communication by assigning clear numeric categories with corresponding management pathways. This clarity helps set expectations and guides next steps, especially in shared decision-making discussions regarding lung cancer screening and follow-up plans.
Clinical Use and Limitations
While Lung-RADS is a valuable tool in the structured assessment of lung screening CTs, clinical judgment remains essential. Patient comorbidities, preferences, and risk factors should always be integrated into decision-making. Additionally, Lung-RADS is not intended to replace diagnostic evaluation for symptomatic patients or nodules discovered incidentally outside of a structured screening program.
This LUNG-rads calculator applies the Lung-RADS criteria to assist in classification and management planning, based on user-provided nodule characteristics and clinical context. Users are encouraged to review the most recent ACR documentation for comprehensive details and guidance.
References:
- American College of Radiology. Lung CT Screening Reporting and Data System (Lung-RADS) v. 2022
- McKee, B. J., Regis, S. M., McKee, A. B., Flacke, S., & Wald, C. (2015). Performance of ACR Lung-RADS in a clinical CT lung screening program. Journal of the American College of Radiology : JACR, 12(3), 273–276.

I could not resist commenting. Exceptionally well written!
Nicely done. So helpful