Fleischner Calculator for Incidental Pulmonary Nodules
Related Calculators
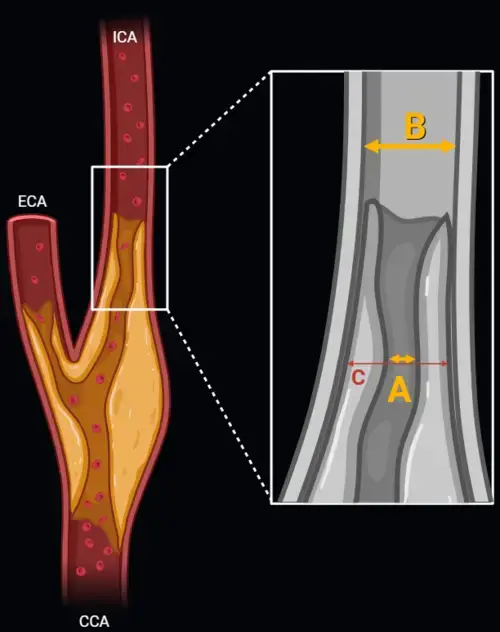
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
Lung cancer screening reporting on CT using standardized Lung-RADS categories and recommendations.

Coronary artery disease reporting on CT angiography using standardized stenosis severity and reporting categories.
Thyroid nodule risk stratification using ultrasound features and ACR TI-RADS scoring system.

More about the Fleischner Criteria Calculator
How to use the Fleischner Criteria Calculator in radiology practice
The Fleischner Criteria Calculator helps structure follow-up decisions for incidentally detected pulmonary nodules on CT by combining nodule size, attenuation pattern, and patient risk profile into practical surveillance pathways. In everyday reporting, it functions as an educational and clinical decision-support tool that can improve consistency in pulmonary nodule follow-up recommendations while preserving the need for radiologist interpretation and patient-specific judgment. The increasing use of multidetector CT has made incidental lung nodule CT findings a routine part of thoracic imaging, which is why standardized follow-up language remains important for both radiologists and referring clinicians. [1]
Clinical application begins with accurate measurement and characterization. Nodule size should be measured using the average of the long-axis and short-axis diameters, rounded to the nearest whole millimeter. Morphology should then be categorized as solid, pure ground-glass, or part-solid, because solid and subsolid nodule management follows different CT-based follow-up strategies. Patient risk also matters, especially the distinction between low-risk versus high-risk patients based on smoking history, carcinogen exposure, and prior lung cancer history. [1]
Fleischner guidelines for incidental pulmonary nodules
The 2017 guideline update shifted management toward more selective surveillance, particularly for smaller nodules, with the goal of reducing unnecessary imaging while maintaining appropriate attention to lesions with higher malignant potential. This approach supports pulmonary nodule risk stratification by emphasizing size thresholds, attenuation characteristics, and clinical context rather than uniform follow-up for every lesion. The result is a more practical framework for imaging surveillance intervals and nodule size-based follow-up in daily radiology workflow. [1]
For many nodules smaller than 8 mm, the probability of malignancy is low, which supports a conservative approach in appropriately selected patients. This is consistent with screening data showing that a large proportion of small nodules do not represent clinically significant cancer, while repeated imaging can increase cumulative radiation exposure and downstream testing. [2]
Key variables for pulmonary nodule risk stratification
Three variables drive management decisions: nodule size, nodule composition, and patient risk. Solid nodules are defined by homogeneous soft-tissue attenuation that obscures underlying lung architecture. Pure ground-glass nodules show hazy increased attenuation with preserved bronchovascular markings. Part-solid nodules contain both ground-glass and solid components, and the size of the solid portion has major implications for escalation of workup. [1]
Risk assessment extends beyond smoking history alone. Upper lobe location, spiculated margins, interval growth, and suspicious internal architecture increase concern even when a lesion falls within a size category that might otherwise suggest routine surveillance. Comparison with prior imaging remains one of the most useful steps in radiologic nodule characterization, because stability or growth can materially change management. [1]
| Nodule category | Low-risk patient | High-risk patient |
|---|---|---|
| Solid nodule < 6 mm | No routine follow-up | Optional CT at 12 months if suspicious morphology or upper lobe location is present |
| Solid nodule 6 to 8 mm | CT at 6 to 12 months, then consider CT at 18 to 24 months | CT at 6 to 12 months, then CT at 18 to 24 months |
| Solid nodule > 8 mm | Consider CT at 3 months, PET/CT, tissue sampling, or a combination depending on clinical context | Consider CT at 3 months, PET/CT, tissue sampling, or a combination depending on clinical context |
| Pure ground-glass nodule < 6 mm | No routine follow-up | No routine follow-up |
| Pure ground-glass nodule ≥ 6 mm | CT at 6 to 12 months to confirm persistence, then every 2 years until 5 years if stable | CT at 6 to 12 months to confirm persistence, then every 2 years until 5 years if stable |
| Part-solid nodule ≥ 6 mm | CT at 3 to 6 months to confirm persistence; if persistent and solid component remains < 6 mm, annual CT until 5 years | CT at 3 to 6 months to confirm persistence; if persistent and solid component remains < 6 mm, annual CT until 5 years |
Solid vs subsolid nodules and follow-up recommendations
Solid nodules are generally managed using size and patient risk as the main decision points. A 6 mm threshold is central to many pulmonary nodule follow-up recommendations, separating many clinically negligible findings from lesions that merit structured surveillance. For nodules larger than 8 mm, management becomes more individualized and may include short-interval CT, PET/CT, biopsy, or multidisciplinary evaluation depending on morphology, growth pattern, and overall clinical context. [1][3]
Subsolid nodules require a different logic because transient inflammatory opacities can mimic neoplasia and because persistent subsolid lesions may reflect the adenocarcinoma spectrum. Ground-glass nodule management therefore prioritizes confirmation of persistence before long-term surveillance is established. In part-solid nodules, the solid component is particularly important, and a larger solid portion increases concern for invasive behavior and need for definitive evaluation. [1]
Nodule size thresholds and surveillance intervals
The Fleischner Criteria Calculator is most useful when applied alongside prior imaging review and careful measurement technique. A diameter increase of 2 mm or more is generally considered meaningful growth in this setting, recognizing the limits of measurement reproducibility. Volume doubling time can also help contextualize change over time, with faster growth patterns raising greater concern for malignancy. These principles support more precise CT lung nodule follow-up recommendations and reduce ambiguity in report language. [1]
When multiple nodules are present, management is usually guided by the most suspicious lesion rather than simply the largest lesion. Suspicious morphology, upper lobe predominance, or a concerning solid component may justify choosing the shorter end of a recommended surveillance range. This is particularly relevant when applying Fleischner guidelines pulmonary nodules recommendations to complex thoracic CT studies. [1][4]
Clinical use of Fleischner criteria in radiology reporting
In practice, these recommendations are most effective when integrated directly into structured reporting or decision support workflows. Clear documentation of nodule type, size, patient risk category, and proposed imaging interval can improve communication with referring clinicians and make recommendations easier to audit over time. This can also create natural internal pathways to related resources such as Lung cancer screening guidelines, Lung-RADS classification system, Pulmonary nodule risk calculators, CT chest interpretation tools, and Other thoracic radiology calculators.
Even with a structured tool, recommendations should still be interpreted in light of age, comorbidities, life expectancy, competing risks, and imaging quality. The calculator supports decision-making, but it does not replace the radiologist's role in correlating morphology, growth, and clinical setting. That balance is especially important when an incidental pulmonary nodule is detected in patients with prior malignancy, suspected infection, or nonstandard risk profiles that may fall outside routine guideline assumptions. [1]
Limitations of Fleischner guideline application
The Fleischner framework is designed for incidental nodules detected on CT in adults and should not be applied indiscriminately to every pulmonary nodule scenario. It is not intended for lung cancer screening populations managed under separate systems, nor does it account for every clinical circumstance such as immunocompromised status, known primary cancer, or clearly infectious processes. These limitations matter because guideline-based surveillance should always be matched to the actual clinical question being addressed. [1][4]
Frequently Asked Questions (FAQs)
What size threshold usually triggers follow-up for an incidental pulmonary nodule?
For many incidentally detected nodules, 6 mm is the key threshold that begins routine follow-up consideration. Smaller solid nodules in low-risk patients often do not require routine surveillance, while management for high-risk patients may be more selective and morphology dependent. [1]
How do Fleischner recommendations differ for solid and subsolid nodules?
Solid nodules are managed mainly by size and patient risk category. Subsolid nodules require confirmation of persistence, and part-solid nodules are further stratified by the size of the solid component because that feature carries important prognostic value. [1]
Who is considered a high-risk patient under the Fleischner approach?
Higher risk generally includes current or former smokers, patients with relevant occupational carcinogen exposure, and those with a personal history of lung cancer. Suspicious morphology and upper lobe location may also increase concern even within the same size category. [1]
When is no routine follow-up recommended for a pulmonary nodule?
No routine follow-up is commonly recommended for solid nodules smaller than 6 mm in low-risk patients and for pure ground-glass nodules smaller than 6 mm in routine incidental settings. Clearly benign features, such as fat-containing hamartoma or benign calcification patterns, may also alter management. [1]
How should multiple pulmonary nodules be managed on CT?
Management usually focuses on the most suspicious nodule rather than treating every lesion independently. Suspicion is based on morphology, growth, attenuation pattern, and clinical setting, which may influence the selected surveillance interval. [1]
References
- MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017;284(1):228-243. doi:10.1148/radiol.2017161659. View source
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395-409. doi:10.1056/NEJMoa1102873. View source
- Borghesi A, Michelini S, Nocivelli G, et al. Solid indeterminate pulmonary nodules less than or equal to 250 mm3: application of the updated Fleischner Society guidelines in clinical practice. Biomed Res Int. 2019;2019:7218258. doi:10.1155/2019/7218258. View source
- Callister ME, Baldwin DR, Akram AR, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax. 2015;70(suppl 2):ii1-ii54. doi:10.1136/thoraxjnl-2015-207168. View source

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
