AAST Kidney Trauma Radiology Score Calculator
References:
- AAST (American Association for the Surgery of Trauma) 2018 guideline for renal injury scoring.
- Organ injury scaling: spleen, liver, and kidney. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, Flint LM, Gennarelli TA, Malangoni MA, Ramenofsky ML, Trafton PG. J Trauma. 1989 Dec;29(12):1664-6.
- Organ injury scaling: spleen and liver (1994 revision). Moore EE, Cogbill TH, Jurkovich GJ, Shackford SR, Malangoni MA, Champion HR. J Trauma. 1995 Mar;38(3):323-4.
Related Calculators:


More About AAST Kidney Trauma Calculator for Renal Injury Grading
This calculator is designed for radiologists, trauma surgeons, urologists, and emergency medicine professionals to assist with consistent assessment of kidney injuries based on the American Association for the Surgery of Trauma (AAST) grading guidelines. Developed independently, it follows the standardized AAST criteria to promote reliable injury classification and communication throughout trauma teams. While not officially endorsed by the AAST, this tool reflects the latest evidence-based grading system as defined in the 2018 revision.
Renal trauma is a vital component of abdominal trauma evaluation, commonly arising from blunt mechanisms such as motor vehicle accidents, falls, and sports, as well as penetrating trauma like gunshot and stab wounds. The AAST Kidney Injury Scale divides renal trauma into five grades, ranging from minor contusions and subcapsular hematomas to catastrophic injuries involving complete devascularization or hilum avulsion. Accurate grading is key for multidisciplinary discussions among radiology, trauma surgery, urology, and critical care, allowing for early intervention when necessary and reducing the risk of complications.
Imaging and Assessment of Renal Trauma
Multiphase CT is the recommended imaging standard for diagnosing and grading kidney injuries. A comprehensive protocol includes non-contrast, arterial, nephrographic, and excretory phases, which enable detection of active bleeding, vascular damage, and collecting system involvement. These imaging findings are central to accurate grading and may affect both immediate management and follow-up. Although MRI can be considered if contrast is contraindicated, it is less commonly used due to availability and longer acquisition times in acute trauma settings.
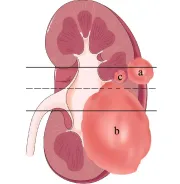
AAST Kidney Injury Scale (2018 Revision)
- Grade I:
- Subcapsular hematoma and/or parenchymal contusion, no laceration
- Grade II:
- Non-expanding perirenal hematoma confined to Gerota fascia
- Laceration ≤1 cm depth, no collecting system involvement
- Grade III:
- Laceration >1 cm depth not involving collecting system
- Contained active bleeding within Gerota fascia
- Grade IV:
- Laceration extending into collecting system with urinary extravasation
- Segmental vascular injury or infarction, renal pelvis disruption
- Bleeding extending outside Gerota fascia
- Grade V:
- Shattered kidney, devascularized kidney, or avulsion of the hilum
- Laceration or thrombosis of main renal artery or vein
Renal Trauma Radiology in Practice
Incorporation of modern CT protocols and AAST grading allows for rapid stratification of injury severity and guides emergency management. Most lower-grade injuries (I-II) and select higher grades (III-IV), especially in stable patients, are managed non-operatively with close observation and supportive care. Studies have shown that nonoperative management can be successful even for some high-grade injuries, provided patients are carefully selected and monitored closely for signs of ongoing bleeding or clinical deterioration. Urology or interventional radiology may be consulted for Grade IV injuries, especially if urinary extravasation or segmental ischemia is present. Surgical intervention is generally reserved for Grade V injuries and for those with hemodynamic instability or other indications.
Other Imaging Considerations
During initial and follow-up imaging, incidental adrenal lesions may be encountered. Although not directly related to acute trauma, tools such as the adrenal washout CT calculator can help with further assessment of these findings, especially when there is diagnostic uncertainty after injury recovery.
Management Guidance Using AAST Grades
- Grades I–II: Nonoperative management with bed rest, hydration, and monitoring is often sufficient.
- Grades III–IV: Observation, potential endovascular intervention or stenting, and multidisciplinary evaluation are generally recommended.
- Grade V: These injuries are typically considered for surgery, including nephrectomy or vascular repair, particularly if instability or ongoing hemorrhage is present.
Tracking outcomes by AAST grade enhances quality assurance and encourages adherence to kidney-preserving strategies, including in pediatric trauma patients whenever feasible.
Benefits of the AAST Kidney Trauma Calculator
This calculator simplifies application of the complex AAST grading system, ensuring rapid and consistent stratification of renal injuries in busy trauma settings. It supports best practices for both trainees and experienced clinicians and helps maintain clear interdisciplinary communication when clinical decisions are time-critical.
Conclusion
Precise grading of renal trauma is fundamental for safe and effective clinical management. Advances in imaging, refinements in the AAST grading scale, and the adoption of automated tools have all contributed to improved, kidney-sparing care. Additional resources, such as adrenal lesion calculators, complement comprehensive evaluation and management of abdominal trauma.
Disclaimer
This calculator is independently developed and is not endorsed by the American Association for the Surgery of Trauma. It is intended as a reference to augment—not replace—clinical judgment and current best practices. Users should always review the latest published AAST guidelines, emerging literature, and local protocols in trauma patient care.
Frequently Asked Questions (FAQ)
- What does the AAST Kidney Injury Scale measure?
It categorizes kidney injuries by imaging findings, focusing on hematoma location, laceration depth, collecting system involvement, and vascular disruption, to guide trauma management. - Can all high-grade kidney injuries be managed without surgery?
Nonoperative management is possible for selected stable patients with high-grade injuries under close monitoring, though surgery may be necessary in cases with ongoing bleeding or instability. - What is the role of multiphasic CT in kidney trauma?
Multiphase CT protocols improve detection of both active bleeding and urinary tract injury, ensuring accurate assessment and grading. - Are pediatric kidney injuries graded the same way?
Yes, the same AAST scale applies in children, although institutions may emphasize kidney-sparing strategies and consult pediatric specialists. - Does this calculator make clinical decisions?
The calculator grades the injury based on imaging, but all treatment decisions should be individualized using clinical judgment and up-to-date guidelines.

PGY-5 Radiology and Nuclear Medicine Resident Physician, UT Southwestern Medical Center, USA
