NI-RADS 2025 Calculator
Please note: This calculator will generate two different NI-RADS scores for neck lymph nodes and the primary site. If the scores don't match, consider the higher one for the final recommendation
References:
- Bunch PM, Aiken AH, Baugnon KL, Bazylewicz M, Chang YS, Hagiwara M, Srinivasan A, Strauss SB, Wicks J, Zander DA, Juliano AF. ACR Neck Imaging Reporting and Data System for MRI Version 2025. J Am Coll Radiol. 2025 Aug 5:S1546-1440(25)00442-9. doi: 10.1016/j.jacr.2025.07.023. Epub ahead of print. PMID: 40754125.
- Aiken, A. H., Rath, T. J., Anzai, Y., Branstetter, B. F., Hoang, J. K., Wiggins, R. H., Juliano, A. F., Glastonbury, C., Phillips, C. D., Brown, R., & Hudgins, P. A. (2018). ACR Neck Imaging Reporting and Data Systems (NI-RADS): A White Paper of the ACR NI-RADS Committee. Journal of the American College of Radiology : JACR, 15(8), 1097–1108. https://doi.org/10.1016/j.jacr.2018.05.006
- Aiken AH, Hudgins PA. Neck Imaging Reporting and Data System. Magn Reson Imaging Clin N Am. 2018;26(1):51-62. doi:10.1016/j.mric.2017.08.004
Related Calculators
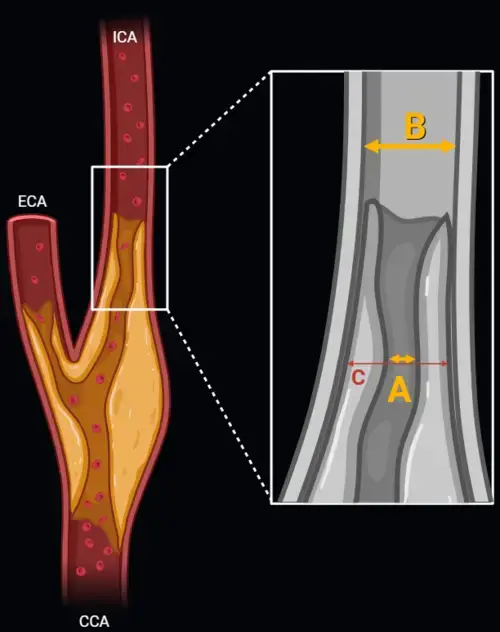
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.

SINS scoring for stability of spine in spinal tumors based on imaging findings and clinical symptoms
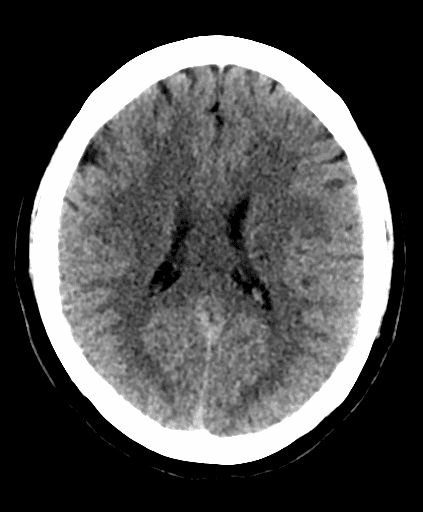
Early ischemic stroke assessment using CT scoring of middle cerebral artery territory involvement.

MRI-based grading of cavernous sinus invasion using the Knosp classification for pituitary tumors
More about the NI-RADS 2025 Calculator
The Neck Imaging Reporting and Data System (NI-RADS™) is a structured surveillance framework developed by the American College of Radiology (ACR) to assist in the interpretation of post-treatment imaging in patients with head and neck cancers. Since its introduction in 2017, NI-RADS™ has played an important role in providing uniform terminology, improving interdisciplinary communication, and supporting evidence-based follow-up strategies for patients undergoing routine cancer surveillance.
This system is specifically tailored for use in individuals with previously treated malignancies involving the upper aerodigestive tract and related structures. NI-RADS™ is compatible with a variety of imaging modalities, including contrast-enhanced CT (CECT), MRI, and hybrid PET/CT or PET/MRI scans, offering flexibility across different diagnostic workflows. By categorizing imaging findings based on recurrence suspicion, it offers practical guidance for managing uncertain or potentially recurrent disease in this complex anatomical region.
NI-RADS™ Categories and Their Implications
NI-RADS™ organizes imaging results into five standardized categories, each reflecting a different level of concern for disease recurrence. These categories are linked with corresponding clinical actions, helping providers tailor surveillance or intervention based on risk level:
- NI-RADS 0: Represents an incomplete assessment due to missing prior imaging, which is necessary for comparison. A definitive category will be assigned once appropriate reference studies become available.
- NI-RADS 1: Indicates no evidence of disease recurrence. Imaging reveals only expected post-treatment changes, and continued routine surveillance is typically advised.
- NI-RADS 2: Suggests low-level suspicion of recurrence. This category is subdivided based on the location and character of findings:
- NI-RADS 2a: Superficial mucosal changes or mild focal uptake on PET imaging. Direct visualization, such as laryngoscopy or endoscopy, is generally recommended.
- NI-RADS 2b: Deep or submucosal changes with mild to moderate radiotracer uptake. Short-term follow-up imaging or further assessment with a different modality may be appropriate.
- NI-RADS 3: Indicates high suspicion for recurrence. Imaging reveals new or enlarging masses, often with intense PET tracer uptake. Biopsy or tissue confirmation is usually warranted.
- NI-RADS 4: Reflects proven disease recurrence, either via pathology or unmistakable radiological and clinical progression. Appropriate treatment decisions should be initiated by the care team.
Applications and Benefits of NI-RADS™
NI-RADS™ offers significant advantages in routine clinical use. By promoting standardized image interpretation and structured reporting, it helps reduce inter-reader variability and enhances consistency across imaging centers. This uniformity is especially important in the multidisciplinary management of patients with head and neck cancers, where precise communication between radiologists, oncologists, surgeons, and primary care providers can influence the timing and nature of subsequent interventions.
The system’s integration of management recommendations within each category allows for more streamlined patient care, supporting appropriate follow-up intervals and minimizing unnecessary imaging or invasive procedures. For institutions involved in data tracking or quality improvement initiatives, NI-RADS™ also facilitates collection of reproducible data for monitoring outcomes and optimizing care pathways.
Importantly, the framework is adaptable to evolving clinical practices and imaging technology. It can be applied consistently across both academic and community settings, helping providers meet surveillance guidelines and coordinate care in accordance with institutional protocols or national best practices.
Use in Multimodal Imaging and Evolving Cancer Care
NI-RADS™ is well-suited for interpreting results from a wide range of modalities, including emerging technologies like PET/MRI. The system can accommodate nuanced findings from different anatomical compartments of the head and neck region, including the primary tumor bed and regional lymph nodes. This flexibility allows radiologists to account for the varied post-treatment anatomy and physiologic changes that may affect interpretation.
By incorporating a risk-stratified structure that guides decision-making, NI-RADS™ helps bridge the gap between diagnostic imaging and clinical action. Its use contributes to thoughtful, individualized follow-up plans that prioritize both thorough surveillance and patient well-being.
To explore more about the NI-RADS™ system, including original ACR documentation, criteria tables, and imaging examples, please visit the American College of Radiology’s official NI-RADS™ page.
