Pulmonary Embolism Severity Index (PESI score) Calculator
Related Calculators

Evaluation of vascular resistance using Doppler ultrasound measurements of systolic and diastolic flow velocities.

Clinical severity assessment of post-thrombotic syndrome using symptom and sign-based Villalta scoring system.
Differentiation of adrenal adenomas using absolute and relative washout measurements on contrast-enhanced CT.
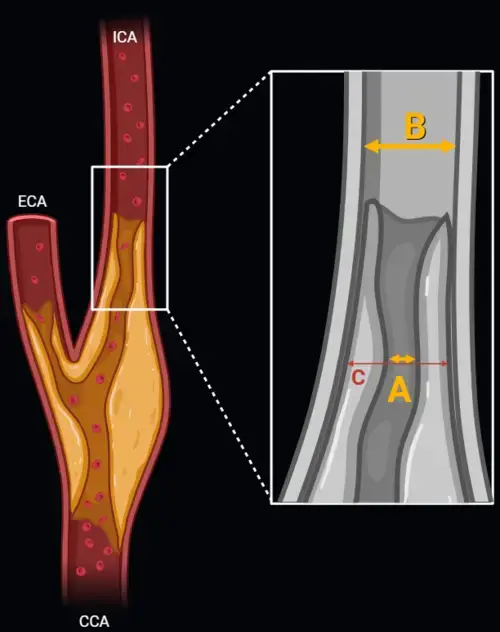
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
More about the PESI Score Calculator
Clinical use of the PESI Score Calculator in acute pulmonary embolism
The PESI Score Calculator supports pulmonary embolism risk stratification in patients with acute PE by estimating short-term mortality risk and helping structure disposition decisions. In routine practice, hemodynamic stability alone does not fully define risk. Many normotensive patients remain appropriate for standard ward admission or outpatient treatment, while others have occult right ventricular dysfunction or evolving physiologic compromise that warrants closer monitoring. Used as a clinical decision-support tool, the PESI Score Calculator helps organize bedside assessment without replacing physician judgment [1][2].
The original Pulmonary Embolism Severity Index was developed to estimate 30-day mortality, not to diagnose PE. Its main value is prognostic classification after PE has been identified. This makes it particularly useful when deciding whether a patient may be considered for outpatient therapy, short inpatient observation, or conventional admission. It also provides a common framework for communication across emergency medicine, hospital medicine, pulmonology, and critical care teams [1][5].
For broader bedside assessment, the score should be interpreted alongside imaging findings, biomarker data, oxygen requirement, bleeding risk, and practical safety factors.
How to calculate the PESI score
The original PESI score calculation uses 11 clinical variables collected from demographics, comorbidity history, vital signs, and mental status examination. Age contributes one point per year, so advancing age strongly influences the final score. Additional weighted variables include male sex, active cancer, heart failure, chronic lung disease, tachycardia, low systolic blood pressure, tachypnea, hypothermia, altered mental status, and oxygen saturation below 90% [1].
Precise interpretation of each variable matters. Altered mental status refers to findings such as disorientation, lethargy, stupor, or coma rather than nonspecific fatigue. Cancer generally refers to active malignancy, including metastatic disease or treatment within the prior 6 months in the original derivation framework. Oxygen saturation should be interpreted in clinical context, including baseline oxygen needs when relevant. Because this is a PE mortality risk score rather than a diagnostic rule, the score is best applied after the diagnosis of acute pulmonary embolism has already been established [5].
PESI score classification and risk categories
After all points are summed, patients are placed into PESI classification classes I to V. Lower classes are associated with lower 30-day mortality, while higher classes identify patients who are more likely to require hospital-based management and closer surveillance. In practice, Classes I and II are commonly considered the low-risk range for outpatient treatment evaluation, provided no major exclusion criteria are present [4][5].
| PESI total points | Risk class | Estimated 30-day mortality | Typical clinical interpretation |
|---|---|---|---|
| ≤65 | Class I | 0.0% to 1.1% | Low risk, outpatient treatment may be considered if other safety criteria are met |
| 66 to 85 | Class II | 1.1% to 3.1% | Low risk, outpatient treatment or early discharge may be considered in selected patients |
| 86 to 105 | Class III | 3.2% to 6.5% | Intermediate risk, inpatient management is often appropriate |
| 106 to 125 | Class IV | 4.0% to 10.4% | Higher risk, inpatient monitoring and further risk assessment are usually needed |
| >125 | Class V | 10.0% to 24.5% | High risk, escalation of monitoring and multidisciplinary evaluation may be required |
PESI versus simplified PESI (sPESI)
The simplified PESI score, or sPESI, reduces the original model to 6 dichotomous variables: age older than 80 years, cancer, chronic cardiopulmonary disease, heart rate at least 110 beats per minute, systolic blood pressure below 100 mmHg, and oxygen saturation below 90%. Each variable contributes 1 point. A simplified PESI score of 0 identifies a lower-risk group, while a score of 1 or more indicates higher risk [2].
The simplified PESI score is often useful when rapid bedside triage is needed. The original PESI provides greater granularity across a wider spectrum of risk, while sPESI offers a more streamlined classification for pulmonary embolism risk stratification. Both approaches are prognostic tools, and both should be integrated with the rest of the clinical picture rather than used in isolation [1][5].
Clinical use of PESI in pulmonary embolism management
Disposition decisions in acute PE usually require more than one layer of assessment. A patient with a low PESI or sPESI may still need admission because of hypoxemia, bleeding risk, severe pain, social barriers, impaired medication access, or concern for early deterioration. Conversely, a patient with favorable physiology, stable oxygenation, and reliable follow-up may be a reasonable candidate for outpatient therapy when low-risk features are present. This is why risk assessment pulmonary embolism pathways often combine mortality scores with practical safety criteria such as the Hestia framework [4].
Important safety considerations before outpatient treatment include hemodynamic stability, absence of active bleeding or major bleeding risk, adequate renal and hepatic function for the planned anticoagulant strategy, stable oxygen requirement, and the ability to obtain medications and return promptly for reassessment. The score helps identify a low-risk cohort, but final disposition still depends on the treating clinician's integrated judgment.
Limitations of PESI scoring
A key limitation of the Pulmonary Embolism Severity Index is that it primarily estimates 30-day mortality and does not directly measure short-term hemodynamic deterioration over the next several hours to days. Some normotensive patients with RV strain, elevated troponin, rising lactate, or worsening oxygen needs may have important near-term risk that is not fully captured by the traditional PESI framework [3].
Recent work on the Pulmonary Embolism Progression score has attempted to address this gap by focusing on early clinical decline in intermediate-risk PE. Variables such as oxygen requirement, lactate, high-sensitivity troponin, severe RV dysfunction, and clot distribution may provide additional insight into short-term progression risk. These models are complementary to, not substitutes for, the established PE severity scoring system used for baseline mortality estimation [3].
Another practical limitation is that age heavily influences the original score. Older adults may be assigned a higher class even when physiologic derangement is limited, while younger patients with concerning RV findings may still require careful inpatient observation despite a lower calculated score. For that reason, PESI score calculation is best viewed as one structured component of a broader clinical assessment.
Frequently Asked Questions (FAQs)
What does the PESI Score Calculator estimate?
It estimates short-term mortality risk after acute pulmonary embolism and helps organize disposition planning. It is a prognostic tool used after PE is diagnosed, not a diagnostic test for PE itself [1][5].
What is the difference between PESI and simplified PESI score (sPESI)?
The original PESI uses 11 weighted variables and places patients into 5 risk classes. The simplified PESI score uses 6 yes or no variables and separates patients into lower-risk and higher-risk groups. The original model provides more granularity, while sPESI is faster at the bedside [1][2].
Can a low PESI score support outpatient treatment?
Yes, low-risk classes may support consideration of outpatient therapy or early discharge, but only when the rest of the clinical picture is favorable. Oxygen requirement, bleeding risk, social support, medication access, and follow-up reliability remain important parts of the decision [4][5].
How is altered mental status defined in PESI score calculation?
In the original model, altered mental status refers to clinically meaningful abnormalities such as disorientation, lethargy, stupor, or coma. Nonspecific malaise or fatigue does not meet that definition [1].
Does the PESI score identify patients at risk of early deterioration?
Not completely. The score is strongest for mortality risk estimation over 30 days. Patients with RV dysfunction, elevated biomarkers, worsening oxygen needs, or other concerning findings may need additional assessment beyond PESI alone [3][5].
References
- Aujesky D, Obrosky DS, Stone RA, et al. Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med. 2005;172(8):1041-1046. doi:10.1164/rccm.200506-862OC. External link
- Jiménez D, Aujesky D, Moores L, et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med. 2010;170(15):1383-1389. doi:10.1001/archinternmed.2010.199. External link
- Ehret J, Wakefield D, Badlam J, et al. Development of the Pulmonary Embolism Progression (PEP) score for predicting short-term clinical deterioration in intermediate-risk pulmonary embolism: a single-center retrospective study. J Thromb Thrombolysis. 2024;58(2):243-253. doi:10.1007/s11239-024-03051-5. External link
- Silva BV, Calé R, Menezes MN, et al. How to predict prognosis in patients with acute pulmonary embolism? Recent advances. Pol Heart J. 2023;81(7-8):700-711. doi:10.33963/KP.a2023.0143. External link
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405. External link

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
