TIRADS Calculator & Report Generator
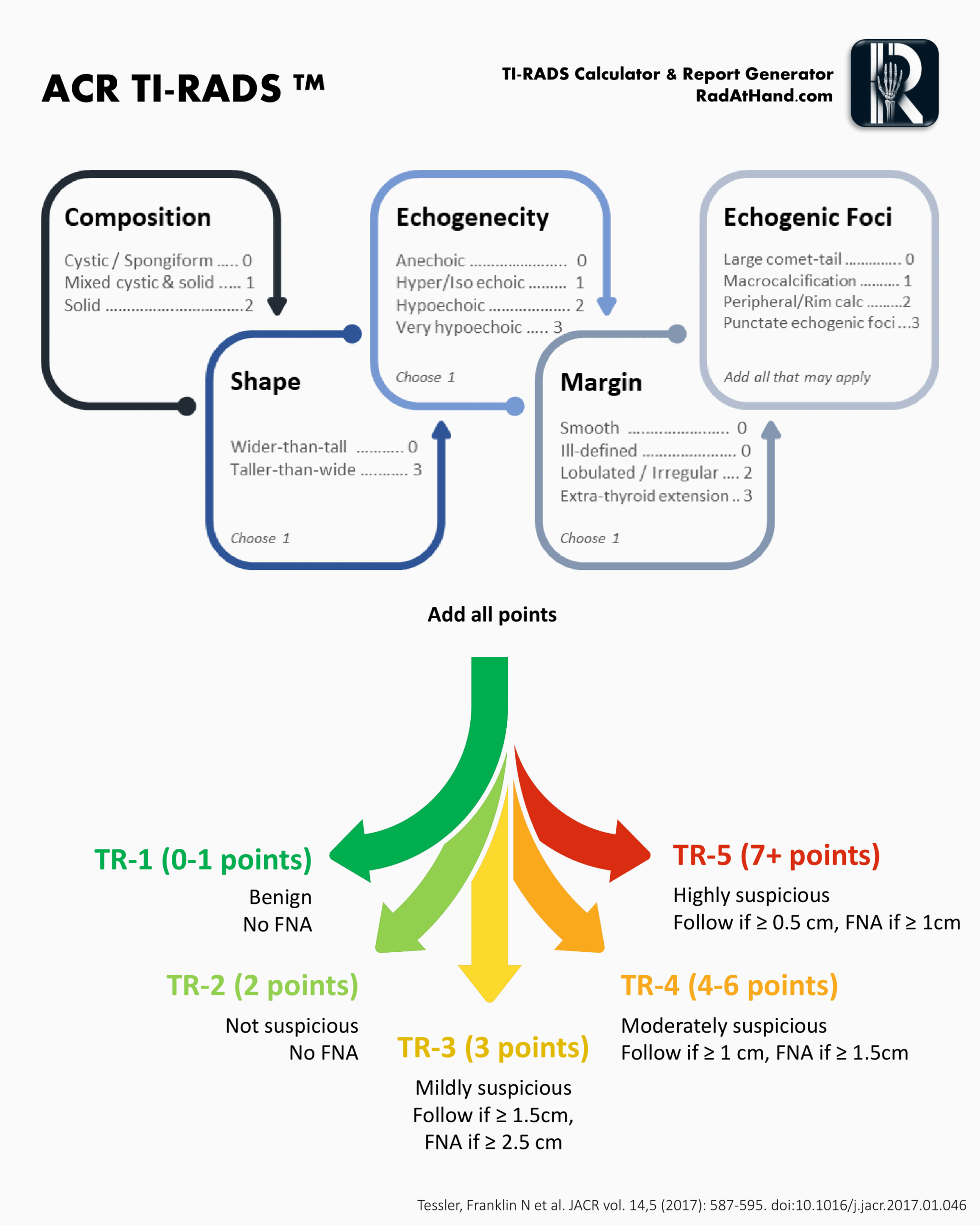
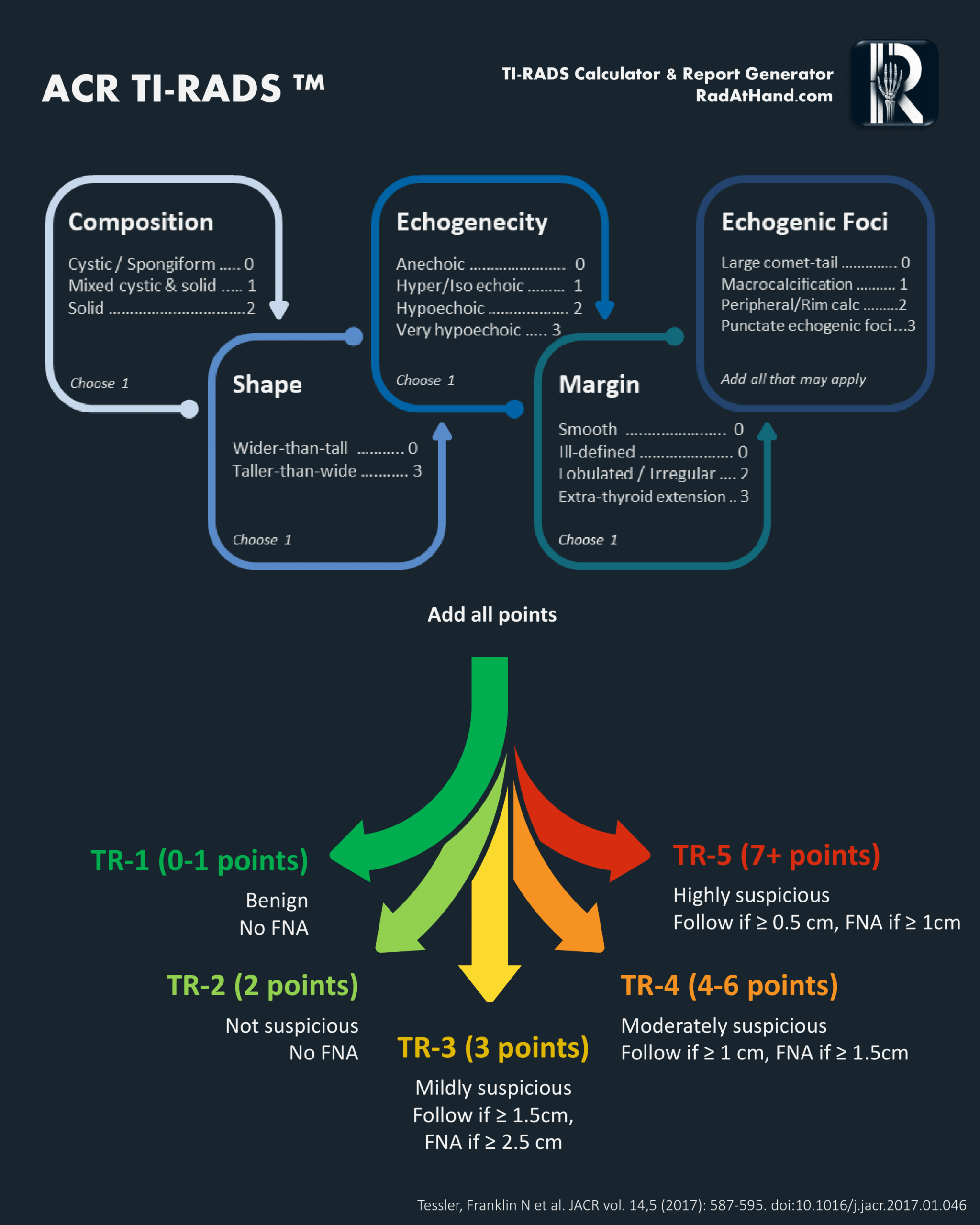
ACR TIRADS flowchart used in this calculator
Related Calculators

Thyroid volume estimation using ultrasound measurements with ellipsoid and WHO-recommended methods.

Ovarian and adnexal lesion risk stratification on ultrasound and MRI using standardized O-RADS categories.

Liver lesion classification for hepatocellular carcinoma risk using CT, MRI, ultrasound, and contrast-enhanced ultrasound.
Differentiation of adrenal adenomas using absolute and relative washout measurements on contrast-enhanced CT.

More about the ACR TIRADS Calculator
This calculator is intended to help practicing radiologists and radiology trainees review thyroid nodule scoring using the American College of Radiology Thyroid Imaging Reporting and Data System, or ACR TIRADS[1]. This thyroid ultrasound scoring system offers a structured way to describe nodule features, assign points, and relate those findings to ACR follow-up and biopsy thresholds. By combining sonographic features into a cumulative score, the calculator mirrors the scoring logic used in ACR TI-RADS and can serve as a practical reference during interpretation and reporting.
The management of thyroid nodules has changed substantially with broader use of standardized ultrasound risk stratification systems. In the setting of very common thyroid nodules on ultrasound, including many incidental or clinically indolent lesions, the TIRADS calculator reflects a standardized point-based framework for estimating category-level malignancy risk and organizing management recommendations[3].
The Five Ultrasound Feature Categories in ACR TI-RADS
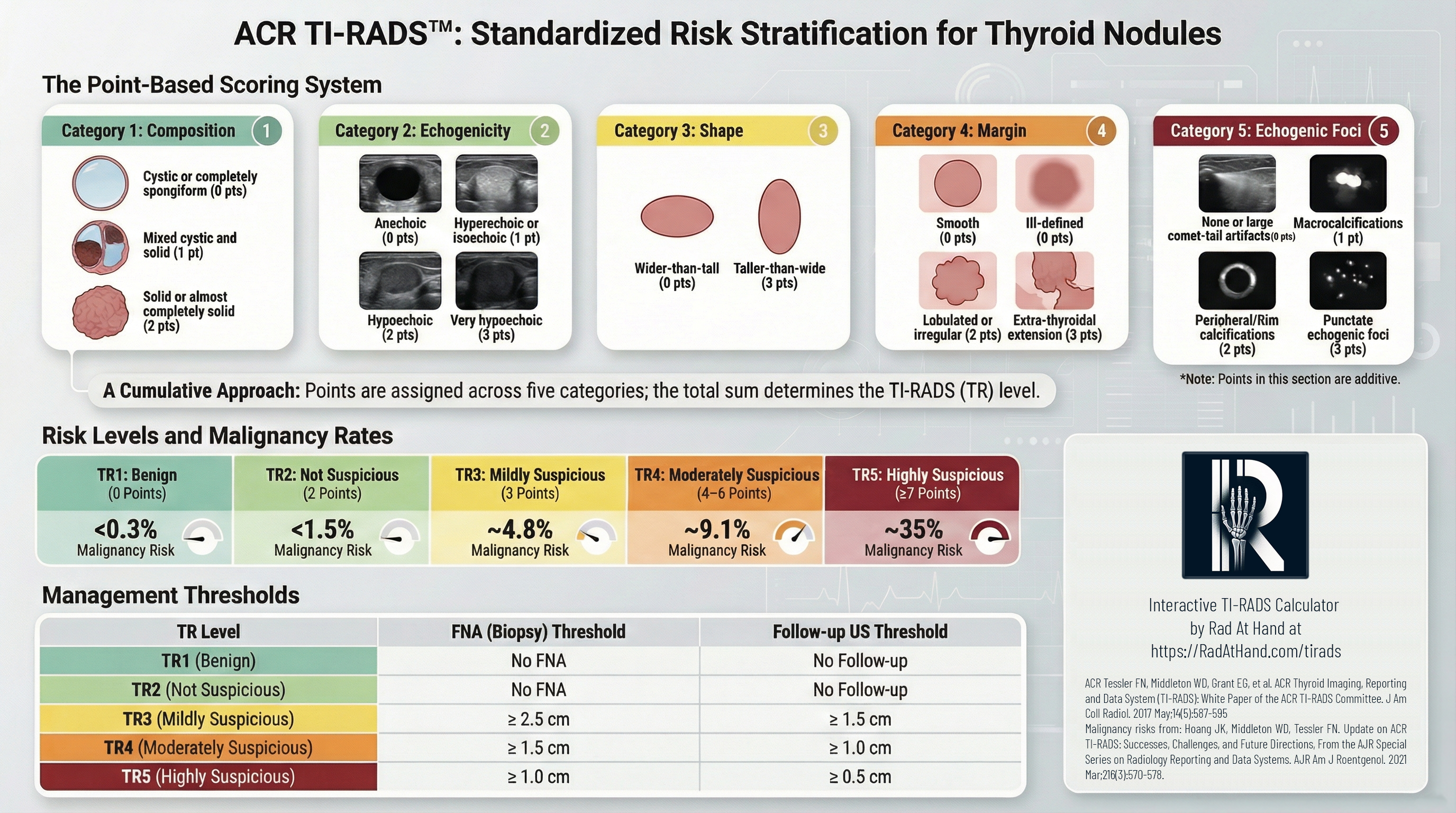
The TIRADS risk assessment derives a cumulative score from five sonographic categories. Points are assigned based on the most suspicious feature in each category[2]. Echogenic foci are the exception, because more than one feature may be present and points in that category are additive.
1. Composition
This category assesses the internal architecture of the nodule.
- Cystic or almost completely cystic (0 points): These lesions are strongly associated with benignity and do not contribute suspicious points in the ACR TI-RADS framework.
- Spongiform (0 points): Defined as composed of greater than 50% small cystic spaces, this appearance is highly specific for benignity.
- Mixed cystic and solid (1 point): This applies regardless of the proportion of the solid component, provided it does not meet spongiform criteria.
- Solid or almost completely solid (2 points): This feature has a higher association with malignancy. For scoring purposes, visual estimation of >95% solid is sufficient.
2. Echogenicity
Echogenicity is evaluated relative to the surrounding thyroid parenchyma and the anterior neck musculature. For mixed nodules, the score is based on the solid component.
- Anechoic (0 points): Applies to cystic fluid.
- Hyperechoic or Isoechoic (1 point): Increased or similar echogenicity relative to thyroid parenchyma.
- Hypoechoic (2 points): Less echogenic than thyroid parenchyma.
- Very Hypoechoic (3 points): Less echogenic than the adjacent strap muscles. This finding is associated with higher suspicion and therefore carries substantial weight in the TI-RADS calculator.
3. Shape
Shape is assessed exclusively in the transverse, or axial, plane.
- Wider-than-tall (0 points): The anteroposterior diameter is less than or equal to the transverse diameter, indicating a parallel orientation.
- Taller-than-wide (3 points): The anteroposterior diameter exceeds the transverse diameter, indicating a non-parallel orientation. This feature is a well-recognized predictor of malignancy in thyroid nodule sonography.
4. Margin
This category evaluates the interface between the nodule and the surrounding tissue.
- Smooth (0 points): Uninterrupted, well-defined border.
- Ill-defined (0 points): The border merges imperceptibly with the thyroid parenchyma. This should be distinguished from an infiltrative margin, because ill-defined margins alone are not considered suspicious in ACR TI-RADS.
- Lobulated or Irregular (2 points): Spiculated or jagged edges, or protrusions into the parenchyma.
- Extrathyroidal Extension (3 points): Frank invasion into adjacent soft tissue or vascular structures. Mere bulging of the capsule does not qualify as extension.
5. Echogenic Foci
Unlike the other categories, multiple features can be selected in this category, and their points are additive.
- None or Large Comet-tail Artifacts (0 points): V-shaped artifacts >1 mm in depth are typically associated with colloid and benignity.
- Macrocalcifications (1 point): Coarse calcifications with posterior acoustic shadowing.
- Peripheral (Rim) Calcifications (2 points): Calcification along the nodule margin. These should be interpreted carefully, especially when dense shadowing obscures the central portion of the nodule.
- Punctate Echogenic Foci (3 points): These are commonly associated with psammomatous calcifications seen in papillary thyroid carcinoma. They are smaller than macrocalcifications and lack the deep V-shaped tail of colloid artifacts.
Clinical Interpretation: TR Categories and Management with the TI-RADS Calculator
The total number of points determines the TI-RADS, or TR, category. This category is associated with an estimated malignancy risk range and corresponding ACR size thresholds for follow-up or fine-needle aspiration.
A notable feature of ACR TI-RADS is its use of relatively higher size thresholds for biopsy than some other systems. This approach reflects the broader goal of reducing overdiagnosis and overtreatment, particularly for indolent lesions, including those affected by the reclassification of Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features, or NIFTP[4].
| Category | Points | Malignancy Risk | Management |
|---|---|---|---|
| TR1: Benign | 0 | < 0.3% | No FNA required. |
| TR2: Not Suspicious | 2 | ~1.5% | No FNA required. |
| TR3: Mildly Suspicious | 3 | ~4.8% | FNA if ≥ 2.5 cm Follow-up US if ≥ 1.5 cm |
| TR4: Moderately Suspicious | 4-6 | ~9.1% | FNA if ≥ 1.5 cm Follow-up US if ≥ 1.0 cm |
| TR5: Highly Suspicious | ≥ 7 | ~35% | FNA if ≥ 1.0 cm Follow-up US if ≥ 0.5 cm |
Frequently Asked Questions (FAQs)
How strictly should size thresholds for FNA be applied?
The size thresholds, 1.5 cm for TR4 and 1.0 cm for TR5, were designed to balance cancer detection with the reduction of overdiagnosis. These thresholds provide a standardized framework, but imaging interpretation still occurs in the setting of the broader clinical picture.
How should partially cystic nodules be scored?
Partially cystic nodules are assigned 1 point for composition as "mixed cystic and solid." Points for echogenicity, margins, and echogenic foci should be based on the solid component or the nodule periphery, as applicable.
How is taller-than-wide shape defined in practice?
This feature is defined as the anteroposterior diameter exceeding the transverse diameter when measured in the axial plane. Measurements from the longitudinal or sagittal plane are not used for this determination in the TI-RADS calculator.
Why does ACR TIRADS Calculator use a point-based system instead of patterns?
The point-based system offers a standardized way to assess sonographic features while weighting findings according to their association with malignancy. This can reduce some of the subjectivity that may arise with best-fit pattern recognition models.
Can TI-RADS be applied to incidental thyroid nodules?
Yes. Once an incidental thyroid nodule has been evaluated with dedicated thyroid ultrasound, ACR TI-RADS can be used to classify the nodule based on its sonographic appearance.
References
- Tessler FN, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017;14(5):587-595.
- Grant EG, et al. Thyroid Ultrasound Reporting Lexicon: White Paper of the ACR Thyroid Imaging, Reporting and Data System Committee. J Am Coll Radiol. 2015;12(12 Pt A):1272-1279.
- Middleton WD, et al. Multi-institutional Analysis of Thyroid Nodule Risk Stratification Using the American College of Radiology Thyroid Imaging Reporting and Data System. AJR Am J Roentgenol. 2017;208(6):1331-1341.
- Nikiforov YE, et al. Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma: A Paradigm Shift to Reduce Overtreatment of Indolent Tumors. JAMA Oncol. 2016;2(8):1023-1029.
All images in this calculator have been obtained from ACR's TI-RADS atlas. Click here to download the full document for TI-RADS from ACR's website.

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA

Hi there,
I just used the TI-RADS calculator for a nodule with the following charactristics:
Nodule #1:
– Location: left lobe (mid segment)
– Size: 0.7 cm
– Composition: Solid or almost completely solid
– Echogenicity: Hypoechoic
– Shape: Wider than tall
– Margins: Smooth
– Additional findings: Peripheral/rim calcifications
And it has classed the nodule as TR 4 rather than 5.
Really appreciate the tool 🙂
Hello Orla,
Thanks for your feedback. Based on the characteristics you listed: solid (2), hypoechoic (2), peripheral/rim calcifications (2), smooth margins (0), wider than tall (0), the total comes to 6 points, which corresponds to TR-4. Could you clarify which feature you counted that led to TR-5?
What an incredibly helpful tool! Thank you!