ASPECTS Calculator for Stroke
ASPECTS for MCA
Click on the infarcted areas to calculate the score.
pc-ASPECTS (Posterior Circulation)
Click on the infarcted areas to calculate the score.
Related Calculators
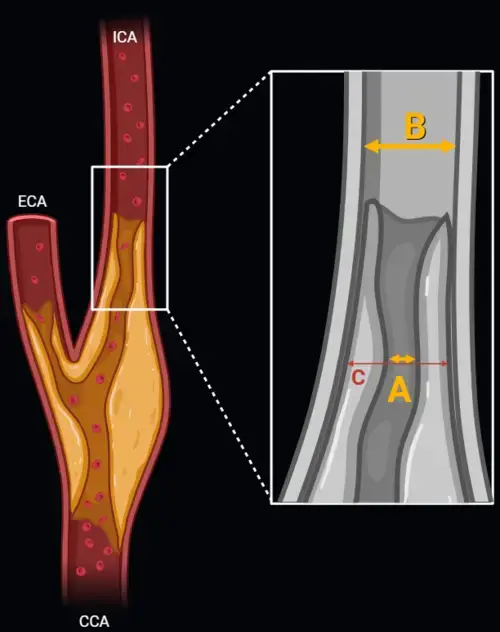
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
Post-treatment head and neck cancer surveillance using CT, MRI, and PET with standardized NI-RADS categories.

Standardized spinal trauma classification based on injury morphology, neurological status, and additional modifiers.
Differentiation of adrenal adenomas using absolute and relative washout measurements on contrast-enhanced CT.
More about the ASPECTS Calculator
ASPECTS Calculator in Acute Ischemic Stroke Imaging
The ASPECTS Calculator is a practical educational and clinical decision-support tool used during acute stroke imaging evaluation to estimate the extent of early ischemic change on noncontrast head CT. In the setting of suspected middle cerebral artery ischemia, it helps structure communication between radiologists, stroke neurologists, emergency physicians, and endovascular teams by translating visually detectei infarct burden into a standardized 10-point stroke imaging score. Used appropriately, it supports rapid large vessel occlusion triage and reperfusion decision-making while remaining complementary to radiologic interpretation and the broader clinical picture.
In modern acute ischemic stroke workflows, standardized early ischemic change detection has become increasingly important. ASPECTS for stroke provides a reproducible framework for MCA territory infarct assessment on baseline CT, especially when urgent treatment decisions must be made before more advanced imaging is available. The score is commonly integrated with CTA findings, clinical severity, and, when indicated, perfusion-based assessment rather than being used in isolation [1][2].
Why the Alberta Stroke Program Early CT Score Matters
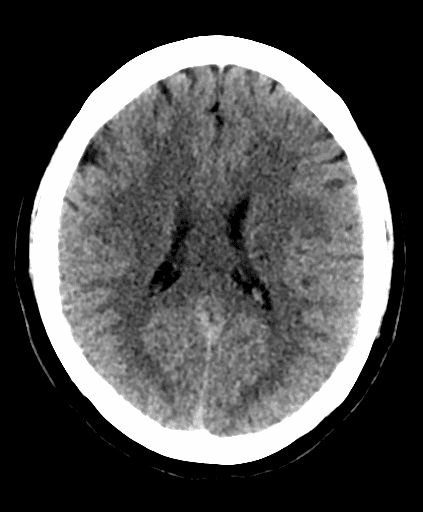
The Alberta Stroke Program Early CT Score is a semiquantitative method for acute ischemic stroke CT scoring within the MCA territory. It was designed to simplify noncontrast CT assessment by dividing the affected vascular territory into 10 predefined regions and subtracting points for early ischemic abnormalities. Typical findings include parenchymal hypoattenuation and loss of gray-white differentiation, which may be subtle during the hyperacute phase.
Clinically, the ASPECTS score is often used as part of infarct burden estimation and treatment triage. In patients with anterior circulation large vessel occlusion, baseline CT ASPECTS frequently contributes to decisions regarding thrombectomy candidacy, particularly when rapid selection is required. Contemporary literature also shows continued interest in patients with lower scores, including those with larger ischemic cores, where endovascular therapy may still offer benefit in selected populations [2].
How to Calculate the ASPECTS Score
The method is straightforward. Begin with a score of 10 on the affected side and subtract 1 point for each region that demonstrates early ischemic change. A score of 10 indicates no visible ischemic abnormality in the scored MCA regions on baseline CT, whereas a score of 0 indicates diffuse involvement across all 10 regions.
This subtraction-based approach makes the ASPECTS Calculator easy to integrate into emergency reporting and multidisciplinary communication. Even so, interpretation requires careful review of subtle density changes, knowledge of the axial levels being assessed, and awareness of common pitfalls in region assignment.
| Axial level | Region | Scoring note |
|---|---|---|
| Ganglionic | Caudate (C) | Subtract 1 point if early ischemic change is present |
| Ganglionic | Lentiform nucleus (L) | Subtract 1 point if early ischemic change is present |
| Ganglionic | Internal capsule (IC) | Subtract 1 point if early ischemic change is present |
| Ganglionic | Insular cortex (I) | Subtract 1 point if early ischemic change is present |
| Ganglionic | M1, anterior MCA cortex | Subtract 1 point if early ischemic change is present |
| Ganglionic | M2, lateral MCA cortex at the insular level | Subtract 1 point if early ischemic change is present |
| Ganglionic | M3, posterior MCA cortex | Subtract 1 point if early ischemic change is present |
| Supraganglionic | M4, anterior MCA cortex | Subtract 1 point if early ischemic change is present |
| Supraganglionic | M5, lateral MCA cortex | Subtract 1 point if early ischemic change is present |
| Supraganglionic | M6, posterior MCA cortex | Subtract 1 point if early ischemic change is present |
| Interpretation | 10 | No scored MCA region shows visible early ischemic change |
| Interpretation | 6 to 9 | More limited ischemic involvement, often relevant to thrombectomy triage in the proper clinical context |
| Interpretation | 3 to 5 | Larger infarct burden, increasingly studied in recent endovascular therapy trials |
| Interpretation | 0 to 2 | Extensive MCA territory involvement |
ASPECTS on Noncontrast CT in Acute Ischemic Stroke
For radiologists, the main challenge is not the arithmetic but the image interpretation. Early ischemic changes can be faint, especially in the insula, deep gray nuclei, and posterior cortical MCA regions. Reader experience affects performance, and interobserver variability remains a known limitation of CT ASPECTS. Published studies have shown that agreement can range from moderate to substantial, depending on reader expertise, region assessed, and how the score is grouped for treatment decisions [1][4][5].
Some investigators have reported improved interobserver agreement with narrower CT window settings, including 8 HU width and 32 HU center, compared with more conventional settings [5]. In practice, window adjustment can be helpful when searching for subtle hypoattenuation, but final interpretation still depends on the full imaging context, side-to-side comparison, and experience with acute stroke imaging evaluation.
Clinical Use of ASPECTS in Stroke Triage and Treatment Decisions
The ASPECTS Calculator is most useful when it is integrated into a broader acute stroke workflow rather than treated as a standalone gatekeeper. In patients with suspected anterior circulation occlusion, the score contributes to rapid communication of infarct burden and may inform discussions regarding thrombectomy, transfer, and the likely extent of established ischemic injury. It is often interpreted alongside CTA, collateral assessment, clinical deficit severity, and, in selected cases, perfusion imaging.
Recent randomized data have expanded interest in thrombectomy for patients with lower ASPECTS values and larger core infarcts. Reviews summarizing RESCUE-Japan LIMIT, SELECT2, ANGEL-ASPECT, and TENSION describe improved outcomes with endovascular therapy in selected large-core stroke populations, although patient selection remains nuanced and imaging interpretation still requires multidisciplinary judgment [2].
Limitations of ASPECTS Scoring
Although ASPECTS is widely used, its limitations are important. The score samples only the MCA territory and does not directly quantify infarct volume. It also simplifies a biologically continuous process into a region-based scale, so two patients with the same score may not have identical infarct distributions or tissue viability. Subtle cortical abnormalities can be missed on baseline CT, and some regions are scored less consistently than others. In a large interobserver study from the TENSION qualification dataset, exact total-score agreement was limited, although agreement improved when patients were grouped into treatment-relevant categories such as 0 to 2, 3 to 5, and 6 to 10 [1].
Another recognized issue is the possibility of imaging-core mismatch in hyperacute referral pathways. Perfusion-based estimates may sometimes overcall irreversible infarction, a concept often referred to as the ghost infarct core. For that reason, stroke imaging interpretation remains strongest when noncontrast CT findings, vascular imaging, clinical status, and treatment timing are considered together rather than relying on a single numeric threshold alone.
ASPECTS Reliability, Prognosis, and Adjunctive Markers
Interest continues to grow in biomarkers and adjunctive tools that may refine prognosis after reperfusion therapy. One example is the Endothelial Activation and Stress Index, or EASIX, calculated as lactate dehydrogenase multiplied by creatinine and divided by platelet count. A recent study reported that higher EASIX values were associated with less favorable 90-day outcomes after mechanical thrombectomy, suggesting a possible link between endothelial dysfunction and reperfusion-related injury [3]. These approaches may add context, but they do not replace structured stroke imaging assessment.
For day-to-day reporting, the most practical role of the ASPECTS Calculator remains consistent, standardized communication. It helps frame early ischemic change scoring, supports multidisciplinary decision-making, and provides a common language across emergency radiology, neuroradiology, vascular neurology, and interventional teams.
Frequently Asked Questions (FAQs)
What does an ASPECTS score of 10 versus 0 mean on noncontrast head CT?
A score of 10 means that none of the 10 scored MCA regions shows visible early ischemic change on the examined side. A score of 0 means that all 10 regions are involved, indicating extensive MCA territory ischemic abnormality.
How is the ASPECTS score calculated in acute stroke imaging?
Start at 10 and subtract 1 point for each ASPECTS region that shows parenchymal hypoattenuation or loss of gray-white differentiation. The method applies to the MCA territory on the affected side and is used to structure acute ischemic stroke CT scoring.
Which ASPECTS regions are most difficult to score reliably?
Interobserver studies suggest that reliability varies by region. The insular cortex is often recognized relatively consistently, while some posterior cortical regions, particularly M3, can be more challenging to score [1].
Can ASPECTS be used for thrombectomy triage?
Yes, but it should be used as part of a broader selection framework. The ASPECTS score is commonly considered alongside vessel imaging, clinical severity, treatment window, and sometimes perfusion imaging when evaluating patients for endovascular therapy [2].
Is MRI more sensitive than CT for early ischemic change detection?
Diffusion-weighted MRI is generally more sensitive for very early ischemic injury than noncontrast CT. However, CT remains central in many acute workflows because it is fast, widely available, and well suited to immediate stroke triage.
References
- van Horn N, Kniep H, Broocks G, et al. ASPECTS interobserver agreement of 100 investigators from the TENSION study. Clin Neuroradiol. 2021;31(4):1093-1100. https://pmc.ncbi.nlm.nih.gov/articles/PMC8648648/
- Lim GZ, Lai YJ, Yeo LLL. Revolutionizing the management of large-core ischaemic strokes: decoding the success of endovascular therapy in the recent stroke trials. J Cardiovasc Dev Dis. 2023;10(12):499. https://pmc.ncbi.nlm.nih.gov/articles/PMC10743836/
- Zhu X, Ma Y, Dong Y, et al. Prognostic value of endothelial activation and stress index in mechanical thrombectomy for patients with acute ischemic stroke. Front Aging Neurosci. 2025;17:1683690. https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2025.1683690/full
- Nimmalapudi S, Inampudi C, Yarlagadda B, et al. Understanding ASPECTS of stroke: inter-rater reliability between emergency medicine physician and radiologist in a rural setup. Neuroradiol J. 2023;36(3):329-334. https://pmc.ncbi.nlm.nih.gov/articles/PMC10268088/
- Kobkitsuksakul C, Tritanon O, Suraratdecha V. Interobserver agreement between senior radiology resident, neuroradiology fellow, and experienced neuroradiologist in the rating of Alberta Stroke Program Early Computed Tomography Score (ASPECTS). Diagn Interv Radiol. 2018;24(2):104-107. https://dirjournal.org/pdf/beb8919b-f013-4ea1-b1c8-40332e840fe1/articles/dir.2018.17336/Diagn%20Interv%20Radiol-24-104-En.pdf

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA

Great
fantastic!