ICH Volume Calculator and Report Generator
Related Calculators
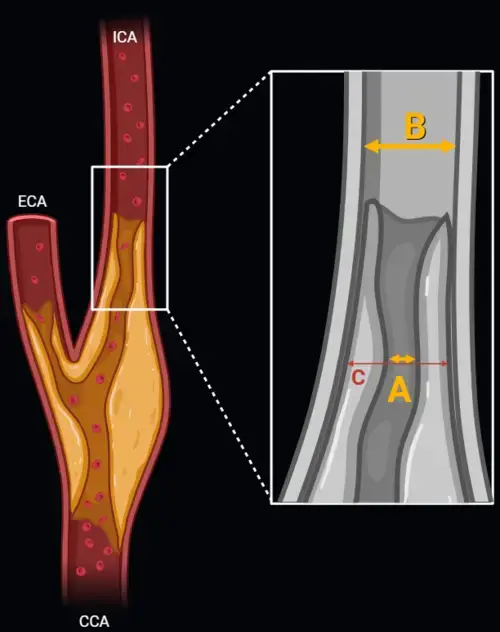
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.
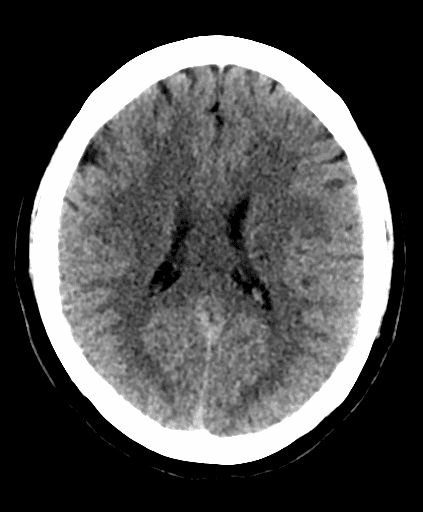
Early ischemic stroke assessment using CT scoring of middle cerebral artery territory involvement.

Standardized spinal trauma classification based on injury morphology, neurological status, and additional modifiers.

MRI-based grading of cavernous sinus invasion using the Knosp classification for pituitary tumors

More about the Intracerebral Hemorrhage Volume Calculator Using ABC/2 and Ellipsoid Methods
The intracerebral hemorrhage volume calculator supports CT-based estimation of parenchymal hematoma volume using the ABC/2 method and an ellipsoid approach. In acute stroke imaging, intracerebral hemorrhage volume is clinically important because baseline hematoma burden is associated with prognosis, early neurologic deterioration, hematoma expansion risk, surgical triage, and communication with neurology, neurosurgery, and neurocritical care teams.[1] The ICH volume calculator should be used as a practical measurement aid, not as a substitute for radiologist interpretation or multidisciplinary clinical judgment.
Why CT Hemorrhage Volume Matters in Acute Stroke Imaging
Noncontrast CT is the usual first-line imaging test for suspected spontaneous intracerebral hemorrhage because it is fast, widely available, and sensitive for acute blood. Hematoma volume CT reporting can help standardize discussions about severity, interval change, mass effect, ventricular extension, and potential need for escalation of care. Volume is also incorporated into prognostic frameworks such as the ICH Score, although such scores should be interpreted carefully and should not be used alone to limit care decisions.[2]
ABC/2 Method for ICH Volume Estimation
The ABC/2 method is a rapid approximation for intracerebral hemorrhage volume estimation on axial CT.[3] Measurement A is the greatest hemorrhage diameter on the axial slice with the largest hematoma area. Measurement B is the greatest diameter perpendicular to A on the same slice. Measurement C represents craniocaudal extent, usually estimated from the number of involved slices multiplied by slice thickness. Some approaches refine C by counting slices with more than 75% of the maximal hematoma area as 1, slices with 25% to 75% as 0.5, and very small areas as 0.
Ellipsoid Hemorrhage Volume and Formula Context
Ellipsoid hemorrhage volume is based on the assumption that the hematoma approximates an ellipsoid. The ellipsoid volume formula can be simplified clinically because the volume of an ellipsoid using three diameters is approximately A × B × C × 0.52. The ABC/2 formula uses a nearby approximation, A × B × C divided by 2, which is convenient for bedside, emergency, and reporting workflows. An ICH volume calculator may present both approaches to help radiologists understand how the estimate was derived.
| Issue | Practical CT consideration |
|---|---|
| Largest axial slice | Use the slice showing the greatest parenchymal hematoma area for A and B measurements. |
| Irregular hematoma shape | Multilobulated or fragmented hemorrhage may reduce the precision of ellipsoid-based estimates. |
| Intraventricular extension | Exclude intraventricular hemorrhage from parenchymal ABC/2 measurement and describe it separately. |
| Slice thickness | Craniocaudal extent depends on slice thickness and slice counting method. |
| Edema and mass effect | Measure hyperdense hematoma, not surrounding edema, while separately reporting mass effect when relevant. |
Practical Reporting Limitations on CT
Manual hemorrhage measurement on CT is an approximation. Accuracy can be affected by irregular margins, mixed attenuation, partial volume effects, adjacent subarachnoid or intraventricular blood, postsurgical change, motion artifact, and posterior fossa anatomy. Supratentorial hemorrhage volume is often easier to estimate than posterior fossa hemorrhage volume because the posterior fossa has smaller compartments, beam hardening artifact, and greater clinical sensitivity to relatively small changes in volume.
For formal reporting, it is often useful to document the estimated parenchymal hematoma volume, measurement method, presence of intraventricular extension, hydrocephalus, midline shift, herniation features, and interval change when prior imaging is available. The intracerebral hemorrhage volume calculator can help maintain consistency, but the final report should reflect the imaging morphology and clinical context.
Frequently Asked Questions (FAQs)
What is the ABC/2 method for intracerebral hemorrhage volume?
The ABC/2 method estimates hematoma volume by multiplying the greatest axial diameter, the perpendicular axial diameter, and the craniocaudal extent, then dividing by 2. It is a rapid approximation for parenchymal intraparenchymal hemorrhage volume on CT.
How is the ABC/2 formula related to ellipsoid hemorrhage volume?
The ABC/2 formula is a simplified approximation of ellipsoid hemorrhage volume. The formal ellipsoid volume formula using three diameters is close to A × B × C × 0.52, while ABC/2 uses A × B × C × 0.5 for clinical convenience.
Should intraventricular hemorrhage be included in an ICH volume calculator?
No. The parenchymal hematoma should be measured separately from intraventricular hemorrhage. Intraventricular extension should be reported because it has independent clinical relevance, especially for hydrocephalus and ventricular obstruction.
When is manual ICH volume estimation less reliable?
Manual ICH volume estimation is less reliable for highly irregular, multilobulated, fragmented, very small, or mixed-density hemorrhages. In these cases, the report can describe the limitation and emphasize the approximate nature of the estimate.
References
- Greenberg SM, Ziai WC, Cordonnier C, et al. 2022 guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2022;53(7):e282-e361. https://www.ahajournals.org/doi/10.1161/STR.0000000000000407
- Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH Score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32(4):891-897. https://www.ahajournals.org/doi/10.1161/01.STR.32.4.891
- Kothari RU, Brott T, Broderick JP, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 1996;27(8):1304-1305. https://www.ahajournals.org/doi/10.1161/01.STR.27.8.1304

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
