Spinal Instability Neoplastic Score (SINS) Calculator for Spinal Tumors
Related Calculators
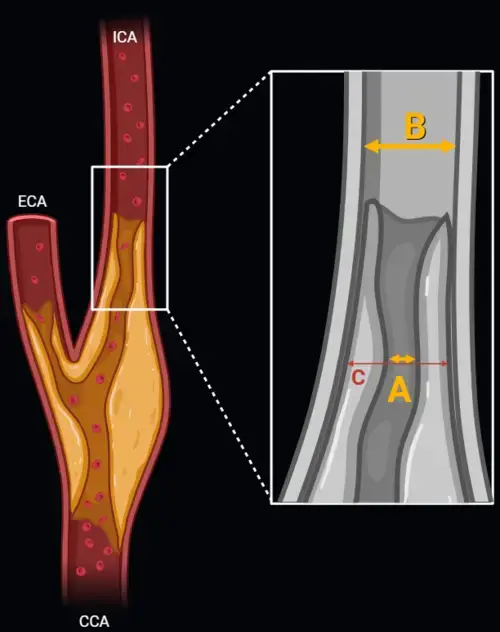
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.

Standardized spinal trauma classification based on injury morphology, neurological status, and additional modifiers.

MRI-based grading of cavernous sinus invasion using the Knosp classification for pituitary tumors
Post-treatment head and neck cancer surveillance using CT, MRI, and PET with standardized NI-RADS categories.

More about the Spinal Instability Neoplastic Scale (SINS) Score Calculator
Purpose of the SINS Score Calculator in Oncology Spine Imaging
The SINS score calculator supports structured assessment of mechanical instability in patients with spinal neoplastic disease. The spinal instability neoplastic scale was developed to help clinicians describe instability risk using a shared clinical and imaging framework, particularly in patients with spine metastases or primary spinal tumors.[1]
In metastatic spine disease stability assessment, the key question is not simply whether tumor is present, but whether tumor-related osseous compromise has reduced the ability of a spinal segment to tolerate physiologic loading. This distinction is clinically important because mechanical pain, deformity, tumor-related vertebral body collapse, and posterior element compromise may affect whether radiation therapy alone is appropriate or whether surgical consultation spine metastases pathways should be considered.
SINS Score Spine Metastases Components and Clinical Meaning
The spinal instability neoplastic scale includes six components: spinal location, mechanical pain, bone lesion quality, radiographic alignment, vertebral body collapse, and posterolateral involvement of spinal elements. One element is clinical, while the remaining elements are primarily radiographic. Together, they provide a structured spinal neoplastic instability assessment without replacing radiologist interpretation, oncologic assessment, or multidisciplinary decision-making.
Location reflects the expected mobility and mechanical stress of each spinal region. Junctional regions, including occiput to C2, C7 to T2, T11 to L1, and L5 to S1, receive higher scores because transition zones are more susceptible to shear forces. Mobile segments such as C3 to C6 and L2 to L4 score higher than semirigid thoracic segments, while rigid sacral levels receive the lowest score.
Mechanical pain is weighted heavily because movement-related pain that improves with recumbency can suggest load-dependent instability. This should be distinguished from biologic tumor pain, radicular pain, or pain from other causes. In practice, the pain component often requires careful clinical correlation, since imaging alone cannot determine whether pain is truly mechanical.
| Component | Scoring options | Imaging or clinical focus |
|---|---|---|
| Location | 0, 1, 2, or 3 | Rigid, semirigid, mobile, or junctional spinal segment |
| Mechanical pain | 0, 1, or 3 | Painless, nonmechanical pain, or movement-related pain relieved by recumbency |
| Bone lesion quality | 0, 1, or 2 | Blastic, mixed, or lytic tumor pattern |
| Spinal alignment | 0, 2, or 4 | Normal alignment, de novo deformity, or subluxation and translation |
| Vertebral body collapse | 0, 1, 2, or 3 | No collapse, greater than 50 percent body involvement, less than 50 percent collapse, or greater than 50 percent collapse |
| Posterolateral involvement | 0, 1, or 3 | No involvement, unilateral involvement, or bilateral involvement of pedicles, facets, or costovertebral joints |
Imaging Interpretation for the Spinal Instability Tumor Score
CT and MRI provide complementary information for the spinal instability tumor score. CT is particularly useful for cortical destruction, lytic versus blastic lesions spine characterization, fracture morphology, posterior element involvement tumor assessment, and subtle collapse. MRI is essential for marrow replacement, epidural tumor extension, neural element compression, paraspinal soft tissue disease, and radiation oncology spine lesions planning.
Bone lesion quality is commonly assessed by CT when available. Lytic disease receives a higher score because it usually reduces osseous structural integrity more than blastic disease. Mixed lesions receive an intermediate score. MRI may show marrow replacement before cortical destruction is obvious, but distinguishing lytic from blastic disease can be more challenging on MRI alone.
Spinal alignment tumor involvement should be assessed for translation, subluxation, kyphosis, scoliosis, or new deformity attributable to tumor. Translation or subluxation carries the highest score within this component because it suggests more advanced mechanical disruption. Vertebral body collapse is evaluated by estimating height loss and the extent of vertebral body involvement. A lesion involving more than half of the vertebral body may receive a score even before measurable collapse occurs.
Score Categories and Clinical Relevance
The total SINS ranges from 0 to 18. Scores of 0 to 6 are generally categorized as stable, 7 to 12 as potentially unstable, and 13 to 18 as unstable.[1] These categories help communicate the degree of concern for mechanical instability spine tumor involvement, but they should be interpreted alongside neurologic status, tumor histology, systemic disease burden, treatment goals, and patient-specific operative risk.
The potentially unstable category is especially important because it includes a heterogeneous group of patients. A patient with mild pain and a small lytic lesion may differ substantially from a patient with progressive deformity and early collapse. For this reason, the SINS score spine metastases category should be viewed as a structured triage and communication tool rather than a rigid treatment directive.
Within multidisciplinary care, SINS may be integrated with frameworks such as NOMS, which considers neurologic, oncologic, mechanical, and systemic factors in metastatic spine disease.[2] In that context, mechanical instability is considered separately from epidural tumor extension or radiosensitivity. A mechanically unstable segment may require surgical evaluation even when tumor histology is expected to respond to radiation.
Limitations of the Spinal Instability Neoplastic Scale
The spinal instability neoplastic scale has practical limitations. Interobserver variability can occur, especially when classifying bone lesion quality, estimating vertebral body involvement, or determining whether pain is truly mechanical. Imaging technique, availability of CT, prior radiation, prior surgery, and diffuse multilevel disease can also complicate scoring.
Multiple spinal lesions should be scored separately rather than summed across levels. The final score should not be used in isolation to determine treatment. Radiologist reporting can be most useful when it clearly describes the imaging features that drive instability concern, including lytic destruction, collapse, deformity, posterior element involvement, and canal or foraminal compromise.
Frequently Asked Questions (FAQs)
What is the SINS score calculator used for?
The SINS score calculator is used to organize clinical and imaging findings related to mechanical instability in spinal neoplastic disease. It helps summarize instability concern in patients with spine metastases or primary spinal tumors.
What are the six components of the spinal instability neoplastic scale?
The six components are spinal location, mechanical pain, bone lesion quality, radiographic alignment, vertebral body collapse, and posterolateral involvement of spinal elements.
What SINS score suggests possible instability in spine metastases?
A score of 7 to 12 is generally considered potentially unstable, while 13 to 18 is generally considered unstable. These categories should prompt clinical correlation and may support referral for surgical evaluation, depending on the overall clinical context.
Is CT or MRI better for calculating the spinal instability tumor score?
Both can be useful. CT is often better for cortical destruction, lytic or blastic lesion characterization, and subtle fracture assessment. MRI is better for marrow involvement, epidural disease, neural compression, and soft tissue tumor extent.
Does SINS replace multidisciplinary spine oncology evaluation?
No. SINS helps structure communication about mechanical stability, but treatment decisions should incorporate neurologic status, tumor biology, systemic disease, patient goals, radiation options, and spine surgery input when appropriate.
References
- Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010;35(22):E1221-E1229. doi:10.1097/BRS.0b013e3181e16ae2
- Laufer I, Rubin DG, Lis E, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. 2013;18(6):744-751. doi:10.1634/theoncologist.2012-0293

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
