Knosp Classification Calculator for Cavernous Sinus Invasion in Pituitary Adenomas
Related Calculators
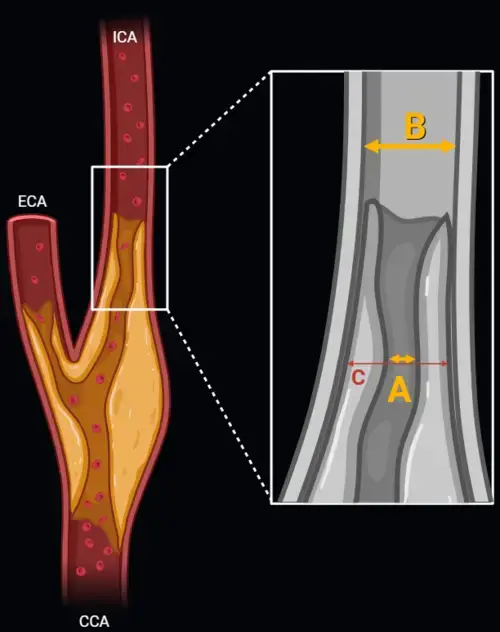
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.

Standardized spinal trauma classification based on injury morphology, neurological status, and additional modifiers.
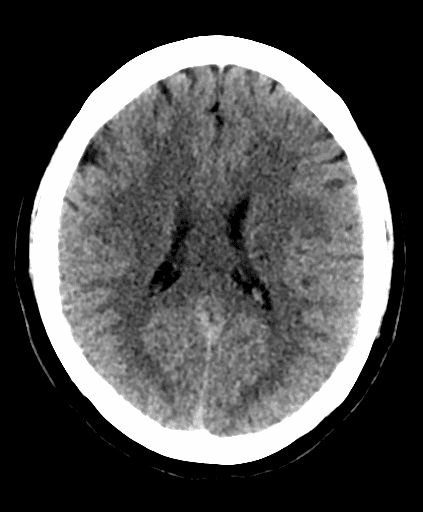
Early ischemic stroke assessment using CT scoring of middle cerebral artery territory involvement.
Post-treatment head and neck cancer surveillance using CT, MRI, and PET with standardized NI-RADS categories.
More about the Knosp Classification Calculator for Cavernous Sinus Invasion by Pituitary Macroadenomas
The Knosp classification calculator is best understood as a structured companion to image interpretation rather than a substitute for it. In the setting of cavernous sinus invasion pituitary macroadenoma assessment, the core task remains careful review of coronal contrast-enhanced MRI, with attention to the relationship between the sellar mass and the intracavernous internal carotid artery.[1][2] For radiologists and skull base surgeons, this grading system offers a common framework for describing parasellar extension, estimating the likelihood of cavernous sinus involvement, and communicating factors that may affect operative strategy and extent of resection.[1][3]
What the Knosp classification measures
The Knosp system was developed to standardize MRI evaluation of pituitary adenoma cavernous sinus invasion by referencing the lateral extent of tumor relative to the intracavernous carotid artery on coronal imaging.[1] In practical terms, the system addresses whether a pituitary macroadenoma MRI demonstrates no meaningful parasellar extension, limited abutment, or more extensive encroachment into the cavernous sinus compartment. Because cavernous sinus invasion often reduces the likelihood of complete resection and may increase technical complexity, the grading system has particular value in preoperative reporting and skull base surgical planning.[3][4]
This is why the language of radiologic grading of pituitary adenoma invasion matters. A report that describes the likely grade, degree of internal carotid artery encasement, and any equivocal findings helps frame the broader multidisciplinary discussion without overstating certainty. Imaging can strongly suggest invasion, but radiologic appearances still need to be interpreted alongside operative findings, endocrinologic status, and overall treatment goals.[2][3]
Knosp classification MRI landmarks and cavernous sinus anatomy pituitary adenoma readers should review
Accurate Knosp classification MRI grading depends on understanding the anatomic landmarks used in the original method. On coronal post-contrast images, three reference lines are drawn relative to the intracavernous and supracavernous carotid segments: the medial tangent line, the line through the carotid centers, and the lateral tangent line.[1] These landmarks provide a reproducible way to describe how far the tumor extends laterally into the parasellar space.
From an imaging perspective, this method reflects a simple but clinically relevant question: is the lesion still medial to the carotid, reaching the intercarotid space, or extending lateral to the artery? In a sellar mass MRI, the answer affects how the radiologist characterizes cavernous sinus extension and whether the surgeon should anticipate a straightforward medial dissection plane or a more complex interface with the cavernous sinus compartment.[1][2]
| Knosp grade | Coronal MRI relationship to carotid landmarks | Typical interpretation points |
|---|---|---|
| Grade 0 | Tumor does not cross the medial tangent line | No convincing lateral parasellar extension on this grading system |
| Grade 1 | Tumor crosses the medial tangent line but does not extend beyond the line through the carotid centers | Limited parasellar extension, invasion is possible but less likely |
| Grade 2 | Tumor extends beyond the carotid center line but not beyond the lateral tangent line | Intermediate category that warrants careful review for additional imaging signs |
| Grade 3 | Tumor extends lateral to the lateral tangent line | Higher likelihood of cavernous sinus involvement; modified systems subdivide this into 3A and 3B |
| Grade 4 | Complete encasement of the intracavernous internal carotid artery | Marked parasellar disease with strong concern for cavernous sinus invasion |
How to interpret the individual grades in daily practice
Grades 0 through 2 are often the most nuanced categories in routine reporting. Grade 0 indicates that the lesion remains medial to the carotid reference line. Grade 1 and Grade 2 reflect increasing lateral extension, but these lower grades do not establish histologic invasion by themselves. They are better viewed as imaging categories that describe tumor position relative to the cavernous sinus rather than absolute proof of medial wall breach.[2][3]
Grades 3 and 4 carry greater clinical weight because they more strongly correlate with surgically recognized cavernous sinus disease and reduced rates of gross total resection.[3][4] In modified descriptions, Grade 3A refers to superior compartment extension and Grade 3B refers to inferior extension below the carotid siphon, a distinction that may matter for endoscopic transsphenoidal surgery and risk discussion with the skull base team.[4] Grade 4, characterized by carotid encasement, usually indicates advanced parasellar invasion and frequently signals limited resectability.
Pituitary adenoma cavernous sinus invasion on MRI, practical interpretation points
When reviewing pituitary adenoma cavernous sinus invasion, coronal contrast-enhanced images are central, but they should not be interpreted in isolation. High-resolution T1 post-contrast images, review of the cavernous sinus compartments, and assessment for preserved venous space between tumor and carotid can improve confidence.[2][3] The presence or absence of a normal pituitary tissue sliver, preserved medial venous compartment, or asymmetric compartment obliteration may help distinguish simple mass effect from more concerning cavernous sinus extension.
Percent carotid encasement can also be useful as an adjunctive descriptor. Meta-analytic data suggest that greater encasement correlates with a higher likelihood of surgical invasion, whereas very limited encasement may help exclude it.[3] For reporting, this means the radiologist can move beyond grade alone and describe whether there is partial carotid contact, broad-based parasellar extension, or more extensive internal carotid artery encasement.
Why the grade matters for skull base surgical planning
The principal clinical relevance of the Knosp system is its relationship to resectability and operative approach. Higher grades are associated with a lower likelihood of complete resection and may influence whether the surgeon anticipates standard exposure, extended exposure, or deliberate residual disease management near critical neurovascular structures.[3][4] This is especially important in patients being considered for endoscopic transsphenoidal surgery, where preoperative understanding of cavernous sinus anatomy, carotid position, and inferior or superior compartment extension can shape the operative corridor.
The report should therefore support decision-making without sounding absolute. A useful approach is to state the likely Knosp grade, describe any parasellar invasion pattern, and note imaging features that either strengthen or weaken concern for true cavernous sinus involvement. This keeps the radiology report clinically helpful while acknowledging that imaging is one part of the broader treatment assessment.
Important limitations and reporting pitfalls
Several pitfalls deserve emphasis. First, MRI may overestimate true invasion, particularly in lower grades where tumor abutment or dural displacement can mimic medial wall transgression.[2][3] Second, image quality, coronal plane selection, and tumor asymmetry can affect grading. Third, the system was designed around carotid line relationships, so unusual tumor morphology or primarily inferior growth may not be fully captured by a simple line-based framework.
More recent literature also highlights distinct patterns of infrasellar and clival spread that create separate surgical challenges and are not summarized by Knosp grade alone.[5] For that reason, a strong report on a pituitary macroadenoma MRI should incorporate both the grade and any additional findings such as sphenoid sinus involvement, clival extension, or atypical growth pattern. A Knosp classification calculator can be used as a quick reference when assigning grade in cases of cavernous sinus invasion by pituitary adenoma, supporting consistent reporting.
Frequently Asked Questions (FAQs)
What does the Knosp classification assess in a pituitary macroadenoma?
It assesses the relationship of the tumor to carotid-based reference lines on coronal MRI in order to estimate the likelihood of cavernous sinus extension or invasion. It is primarily an imaging communication tool used in preoperative assessment.[1][3]
How are Knosp grades 0 through 4 defined on MRI?
The grades are based on whether the tumor remains medial to the medial tangent line, extends to the carotid center line, reaches the lateral tangent line, passes lateral to that line, or completely encases the intracavernous carotid artery.[1]
Why is the Knosp classification important for surgical planning?
It helps surgeons anticipate resectability, operative complexity, and the likelihood of tumor within or beyond the medial cavernous sinus boundary. This can affect preoperative counseling and planning for skull base exposure.[3][4]
What are common MRI pitfalls when grading pituitary adenoma cavernous sinus invasion?
Common pitfalls include relying on a single coronal slice, mistaking compression for invasion, underappreciating preserved venous compartments, and failing to describe additional growth patterns such as clival or sphenoid extension that are not fully captured by grade alone.[2][5]
References
- Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery. 1993;33(4):610-617.
- Cottier JP, Destrieux C, Brunereau L, et al. Cavernous sinus invasion by pituitary adenoma: MR imaging. Radiology. 2000;215(2):463-469. doi:10.1148/radiology.215.2.r00ap18463.
- Dhandapani S, Singh H, Negm HM, et al. Cavernous sinus invasion in pituitary adenomas: systematic review and pooled data meta-analysis of radiological criteria and comparison of endoscopic and microscopic surgery. J Neurosurg. 2016;124(6):1629-1639.
- Micko ASG, Wöhrer A, Wolfsberger S, Knosp E. Invasion of the cavernous sinus space in pituitary adenomas: endoscopic verification and its correlation with an MRI-based classification. J Neurosurg. 2015;122(4):803-811.
- Sannwald LW, Kreße N, Grübel N, et al. Pituitary neuroendocrine tumors extending primarily below the sella and into the clivus: a distinct growth pattern with specific challenges. Curr Oncol. 2026;33(1):36.

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
