MELD 3.0 Calculator
Related Calculators
Pulmonary embolism risk stratification using clinical parameters to estimate mortality and guide management decisions

Clinical severity assessment of post-thrombotic syndrome using symptom and sign-based Villalta scoring system.
Differentiation of adrenal adenomas using absolute and relative washout measurements on contrast-enhanced CT.
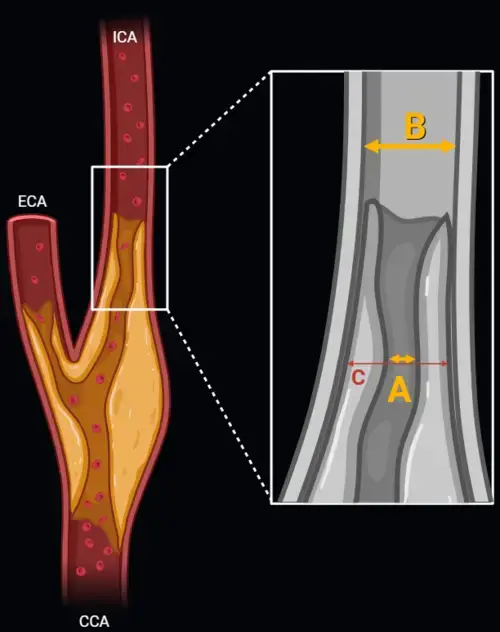
Carotid artery stenosis measurement using NASCET and ECST methods on CT angiography or MR angiography.

More about the MELD 3.0 Calculator for Score Liver Disease Assessment
Clinical Purpose of MELD 3.0 in Liver Disease Severity Assessment
The MELD 3.0 calculator estimates medical urgency in patients with advanced chronic liver disease using the updated Model for End-Stage Liver Disease equation. In clinical practice, the MELD score is used to summarize short-term mortality risk and inform liver transplant prioritization, while remaining only one component of hepatology and transplant decision-making.[1]
MELD 3.0 was developed as an update to prior MELD and MELD-Na models. Earlier MELD scoring incorporated bilirubin, INR, and creatinine, with MELD-Na adding serum sodium to reflect the prognostic importance of hyponatremia. MELD 3.0 retains these core variables, adds serum albumin, incorporates a sex adjustment, and includes interaction terms that better reflect relationships between hepatic dysfunction, renal function, and systemic physiology.[1]
MELD 3.0 Formula and Included Clinical Variables
The MELD 3.0 calculator applies the following equation in adult candidates at least 18 years of age at registration:
MELD 3.0 = 1.33 × (Female) + 4.56 × ln(bilirubin) + 0.82 × (137 − sodium) − 0.24 × (137 − sodium) × ln(bilirubin) + 9.09 × ln(INR) + 11.14 × ln(creatinine) + 1.85 × (3.5 − albumin) − 1.83 × (3.5 − albumin) × ln(creatinine) + 6
For candidates aged at least 12 years who were less than 18 years old at the time of registration, the equation is similar but excludes the sex coefficient and uses a different constant term.
The model incorporates bilirubin, INR, creatinine, sodium, albumin, and sex, with interaction terms involving sodium with bilirubin and albumin with creatinine. These inputs reflect hepatic excretory function, synthetic capacity, renal dysfunction, circulatory physiology, and nutritional or inflammatory status.
| Variable | Clinical relevance |
|---|---|
| Total bilirubin | Reflects hepatic excretory function and hepatocellular or cholestatic dysfunction. |
| INR | Represents impaired hepatic synthetic function and coagulation factor production. |
| Creatinine | Captures renal dysfunction, which is strongly associated with short-term mortality risk in cirrhosis. |
| Sodium | Reflects hyponatremia and circulatory dysfunction associated with portal hypertension. |
| Albumin | Provides information about synthetic function, inflammation, and nutritional reserve. |
| Sex adjustment | Accounts for differences in creatinine-based estimation of renal function across patient groups. |
Implementation Details and Calculator Assumptions
The MELD 3.0 calculator applies standard constraints to maintain physiologic consistency and avoid mathematical distortion:
- Serum bilirubin, INR, and creatinine values below 1.0 are set to 1.0 before logarithmic transformation.
- Serum sodium is limited to a range of 125 to 137 mEq/L.
- Serum albumin is limited to a range of 1.5 to 3.5 g/dL.
- Serum creatinine is capped at 3.0 mg/dL.
- Patients receiving two or more dialysis treatments within 7 days, or continuous renal replacement therapy, are assigned a creatinine value of 3.0 mg/dL.
- The final MELD 3.0 score is rounded to the nearest integer.
The calculator accepts physiologic input ranges for validation, including sodium (100–200 mEq/L), bilirubin (0–60 mg/dL), INR (0.5–20), creatinine (0.01–40 mg/dL), and albumin (0.5–9.9 g/dL), but applies the above constraints during score calculation. The minimum supported age is 12 years.
3-Month Mortality and Survival Estimation
The MELD 3.0 score can be used to estimate short-term survival probability using the following relationship:
Estimated 90-day survival = 0.946exp(0.17698 × MELD − 3.56) × 100
This estimate represents a population-based approximation of survival probability rather than an individualized prediction. Clinical interpretation should consider dynamic changes in laboratory values and the broader clinical context.
Liver Transplant MELD Score Interpretation in Clinical Context
The MELD score is interpreted as a continuous estimate of short-term mortality risk rather than a categorical diagnosis. Higher scores generally reflect greater medical urgency, but interpretation should be integrated with clinical trajectory, complications of portal hypertension, renal function, infection status, and transplant center evaluation.
In practice, MELD-based allocation operates within the UNOS framework alongside exception pathways, tumor-specific criteria, surgical candidacy, and multidisciplinary review.[2]
How MELD 3.0 Differs From MELD-Na
Compared with MELD-Na, MELD 3.0 incorporates serum albumin, includes a sex-based adjustment, modifies coefficient weighting, and introduces interaction terms. These changes were designed to better reflect contemporary cirrhosis risk stratification.[1]
Limitations of MELD Score Liver Disease Assessment
MELD 3.0 does not fully capture frailty, sarcopenia, functional decline, quality of life, refractory symptoms, or all etiologies of hepatic decompensation. Certain clinical conditions may carry risk that is not fully reflected by laboratory variables alone.
The MELD 3.0 model should be viewed as a structured risk estimate within a broader clinical workflow rather than a substitute for hepatology evaluation or transplant selection processes.
Frequently Asked Questions (FAQs)
What is the MELD 3.0 calculator used for?
The MELD 3.0 calculator estimates short-term mortality risk in advanced liver disease and is used in transplant prioritization frameworks. Results should be interpreted within the broader clinical context.
Which variables are included in the MELD 3.0 formula?
The MELD 3.0 formula includes bilirubin, INR, creatinine, sodium, albumin, sex, and interaction terms involving these variables.
How is MELD 3.0 different from MELD-Na?
MELD 3.0 adds albumin, includes a sex adjustment, and uses interaction terms that are not present in MELD-Na.
Does MELD 3.0 predict individual patient outcomes?
No. MELD 3.0 provides a population-based estimate of short-term risk and should not be used as a standalone predictor for individual outcomes.
References
- Kim WR, Mannalithara A, Heimbach JK, et al. MELD 3.0: The Model for End-Stage Liver Disease Updated for the Modern Era. Gastroenterology. 2021;161(6):1887-1895. doi:10.1053/j.gastro.2021.08.050.
- Organ Procurement and Transplantation Network. Liver allocation policies and MELD-based prioritization.

PGY-5 Radiology and Nuclear Medicine Resident Physician
UT Southwestern Medical Center, USA
